

Association of Socioeconomic Status With Risk Factor Target Achievements and Use of Secondary Prevention After Myocardial Infarction
- PMID: 33688966
- PMCID: PMC7948055
- DOI: 10.1001/jamanetworkopen.2021.1129
Association of Socioeconomic Status With Risk Factor Target Achievements and Use of Secondary Prevention After Myocardial Infarction
Abstract
Importance: Low socioeconomic status (SES) is associated with poor long-term prognosis after myocardial infarction (MI). Plausible underlying mechanisms have received limited study.
Objective: To assess whether SES is associated with risk factor target achievements or with risk-modifying activities, including cardiac rehabilitation programs, monitoring, and drug therapies, during the first year after MI.
Design, setting, and participants: This cohort study included a population-based consecutive sample of 30 191 one-year survivors of first-ever MI who were 18 to 76 years of age, resided in the general community in Sweden, were followed up until their routine 11- to 15-month revisit, and were registered in the national registry Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies (SWEDEHEART) from 2006 through 2013. Data analyses were performed from January to August 2020.
Exposure: Individual-level SES by proxy disposable income quintile. Secondary exposures were educational level and marital status.
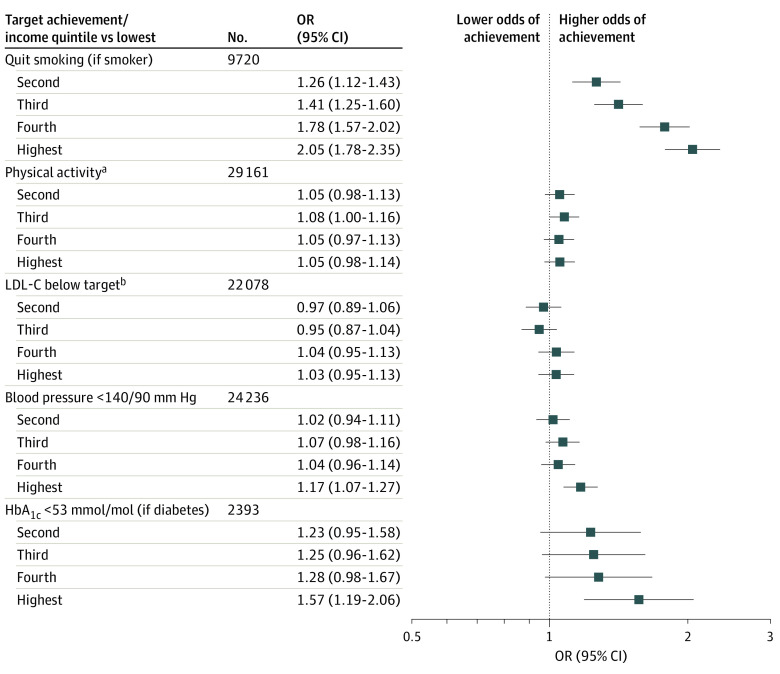
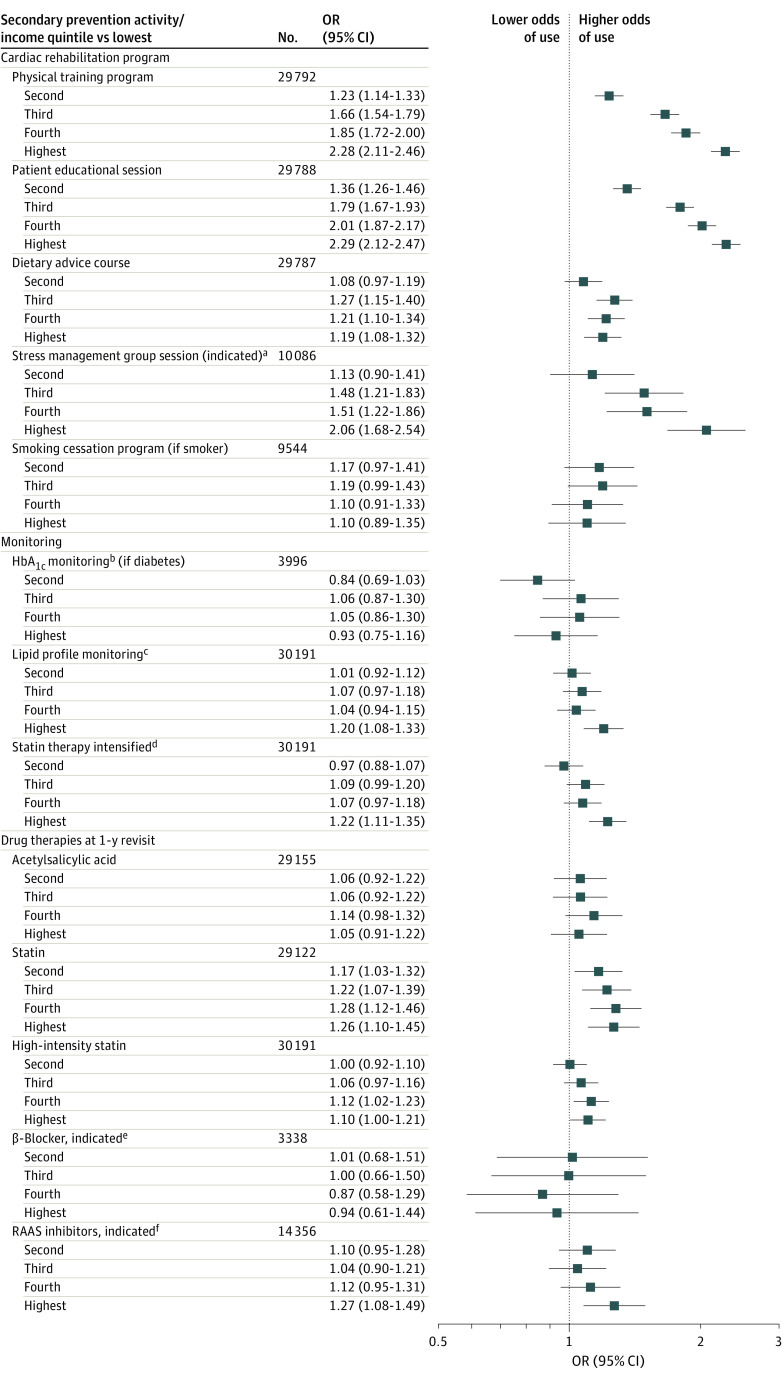
Main outcomes and measures: Odds ratios (ORs) with 95% CIs for achieved risk factor targets at the 1-year revisit and for use of guideline-recommended secondary prevention activities.
Results: The study comprised 30 191 participants (72.9% men) with a mean (SD) age of 63.0 (8.6) years. Overall, higher SES was associated with better target achievements and use of most secondary prevention. The highest (vs lowest) income quintile was associated with achieved smoking cessation (OR, 2.05; 95% CI, 1.78-2.35), target blood pressure levels (OR, 1.17; 95% CI, 1.07-1.27), and glycated hemoglobin levels (OR, 1.57; 95% CI, 1.19-2.06). The highest-income quintile was associated not only with participation in physical training programs (OR, 2.28; 95% CI, 2.11-2.46) and patient educational sessions (OR, 2.29; 95% CI, 2.12-2.47) in cardiac rehabilitation but also with more monitoring of lipid profiles (OR, 1.20; 95% CI, 1.08-1.33) and intensification of statin therapy (OR, 1.22; 95% CI, 1.11-1.35) during the first year after MI. One year after MI, the highest-income quintile was associated with persistent use of statins (OR, 1.26; 95% CI, 1.10-1.45), high-intensity statins (OR, 1.10; 95% CI, 1.00-1.21), and renin-angiotensin-aldosterone system inhibitors (OR, 1.27; 95% CI, 1.08-1.49).
Conclusions and relevance: Findings indicated that, in a publicly financed health care system, higher SES was associated with better achievement of most risk factor targets, programs aimed at lifestyle change, and evidence-based drug therapies after MI. Observed differences in secondary prevention activity may be a factor in higher long-term risk of recurrent disease among individuals with low SES.
Conflict of interest statement
Figures
References
-
- Piepoli MF, Hoes AW, Agewall S, et al. ; Authors/Task Force Members . 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis. 2016;252:207-274. doi:10.1016/j.atherosclerosis.2016.05.037 - DOI - PubMed
-
- Eckel RH, Jakicic JM, Ard JD, et al. ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25, pt B):2960-2984. doi:10.1016/j.jacc.2013.11.003 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
