

Risk Factors Associated With SARS-CoV-2 Seropositivity Among US Health Care Personnel
- PMID: 33688967
- PMCID: PMC7948059
- DOI: 10.1001/jamanetworkopen.2021.1283
Risk Factors Associated With SARS-CoV-2 Seropositivity Among US Health Care Personnel
Abstract
Importance: Risks for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection among health care personnel (HCP) are unclear.
Objective: To evaluate the risk factors associated with SARS-CoV-2 seropositivity among HCP with the a priori hypothesis that community exposure but not health care exposure was associated with seropositivity.
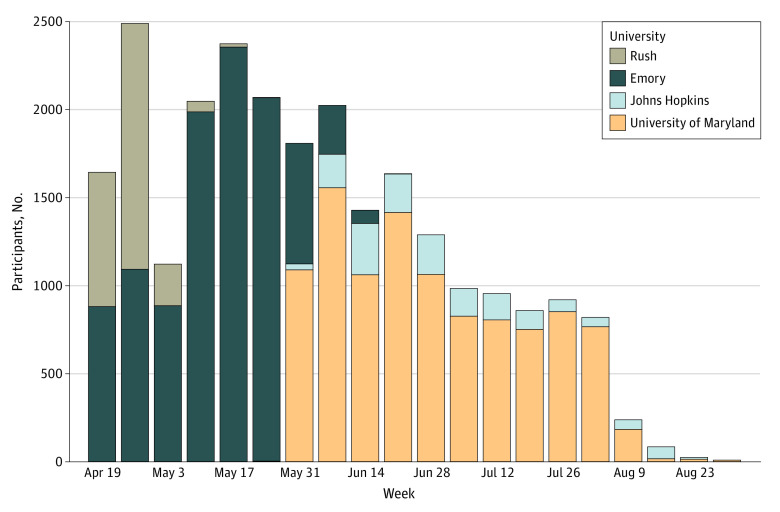
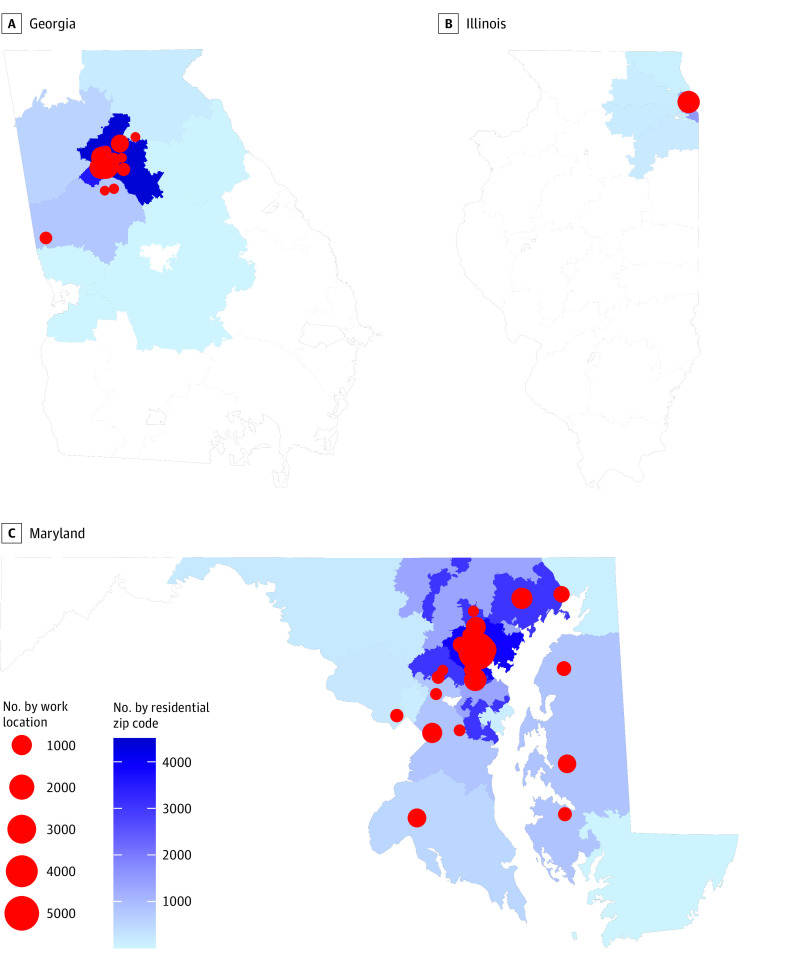
Design, setting, and participants: This cross-sectional study was conducted among volunteer HCP at 4 large health care systems in 3 US states. Sites shared deidentified data sets, including previously collected serology results, questionnaire results on community and workplace exposures at the time of serology, and 3-digit residential zip code prefix of HCP. Site-specific responses were mapped to a common metadata set. Residential weekly coronavirus disease 2019 (COVID-19) cumulative incidence was calculated from state-based COVID-19 case and census data.
Exposures: Model variables included demographic (age, race, sex, ethnicity), community (known COVID-19 contact, COVID-19 cumulative incidence by 3-digit zip code prefix), and health care (workplace, job role, COVID-19 patient contact) factors.
Main outcome and measures: The main outcome was SARS-CoV-2 seropositivity. Risk factors for seropositivity were estimated using a mixed-effects logistic regression model with a random intercept to account for clustering by site.
Results: Among 24 749 HCP, most were younger than 50 years (17 233 [69.6%]), were women (19 361 [78.2%]), were White individuals (15 157 [61.2%]), and reported workplace contact with patients with COVID-19 (12 413 [50.2%]). Many HCP worked in the inpatient setting (8893 [35.9%]) and were nurses (7830 [31.6%]). Cumulative incidence of COVID-19 per 10 000 in the community up to 1 week prior to serology testing ranged from 8.2 to 275.6; 20 072 HCP (81.1%) reported no COVID-19 contact in the community. Seropositivity was 4.4% (95% CI, 4.1%-4.6%; 1080 HCP) overall. In multivariable analysis, community COVID-19 contact and community COVID-19 cumulative incidence were associated with seropositivity (community contact: adjusted odds ratio [aOR], 3.5; 95% CI, 2.9-4.1; community cumulative incidence: aOR, 1.8; 95% CI, 1.3-2.6). No assessed workplace factors were associated with seropositivity, including nurse job role (aOR, 1.1; 95% CI, 0.9-1.3), working in the emergency department (aOR, 1.0; 95% CI, 0.8-1.3), or workplace contact with patients with COVID-19 (aOR, 1.1; 95% CI, 0.9-1.3).
Conclusions and relevance: In this cross-sectional study of US HCP in 3 states, community exposures were associated with seropositivity to SARS-CoV-2, but workplace factors, including workplace role, environment, or contact with patients with known COVID-19, were not. These findings provide reassurance that current infection prevention practices in diverse health care settings are effective in preventing transmission of SARS-CoV-2 from patients to HCP.
Conflict of interest statement
Figures
Comment in
-
Community COVID-19 Incidence and Health Care Personnel COVID-19 Seroprevalence.JAMA Netw Open. 2021 Mar 1;4(3):e211575. doi: 10.1001/jamanetworkopen.2021.1575. JAMA Netw Open. 2021. PMID: 33688960 No abstract available.
References
-
- Jespersen S, Mikkelsen S, Greve T, et al. SARS-CoV-2 seroprevalence survey among 17,971 healthcare and administrative personnel at hospitals, pre-hospital services, and specialist practitioners in the Central Denmark Region. Clin Infect Dis. 2020;ciaa1471. doi: 10.1093/cid/ciaa1471 - DOI - PMC - PubMed
-
- Self WH, Tenforde MW, Stubblefield WB, et al. ; CDC COVID-19 Response Team; IVY Network . Seroprevalence of SARS-CoV-2 among frontline health care personnel in a multistate hospital network—13 academic medical centers, April-June 2020. MMWR Morb Mortal Wkly Rep. 2020;69(35):1221-1226. doi: 10.15585/mmwr.mm6935e2 - DOI - PMC - PubMed
-
- Hunter BR, Dbeibo L, Weaver CS, et al. Seroprevalence of severe acute respiratory coronavirus virus 2 (SARS-CoV-2) antibodies among healthcare workers with differing levels of coronavirus disease 2019 (COVID-19) patient exposure. Infect Control Hosp Epidemiol. 2020;41(12):1441-1442. doi: 10.1017/ice.2020.390 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
