

Early combination of albumin with crystalloids administration might be beneficial for the survival of septic patients: a retrospective analysis from MIMIC-IV database
- PMID: 33689042
- PMCID: PMC7947075
- DOI: 10.1186/s13613-021-00830-8
Early combination of albumin with crystalloids administration might be beneficial for the survival of septic patients: a retrospective analysis from MIMIC-IV database
Abstract
Background: Fluid therapy is a cornerstone in the treatment of sepsis. Recently, the guidelines have recommended the combined administration that using crystalloids plus albumin for septic patients, but the optimal timing for albumin combined is still unclear. The objective of this study was to investigate the association of timing of albumin combined with 28-day mortality in patients with sepsis.
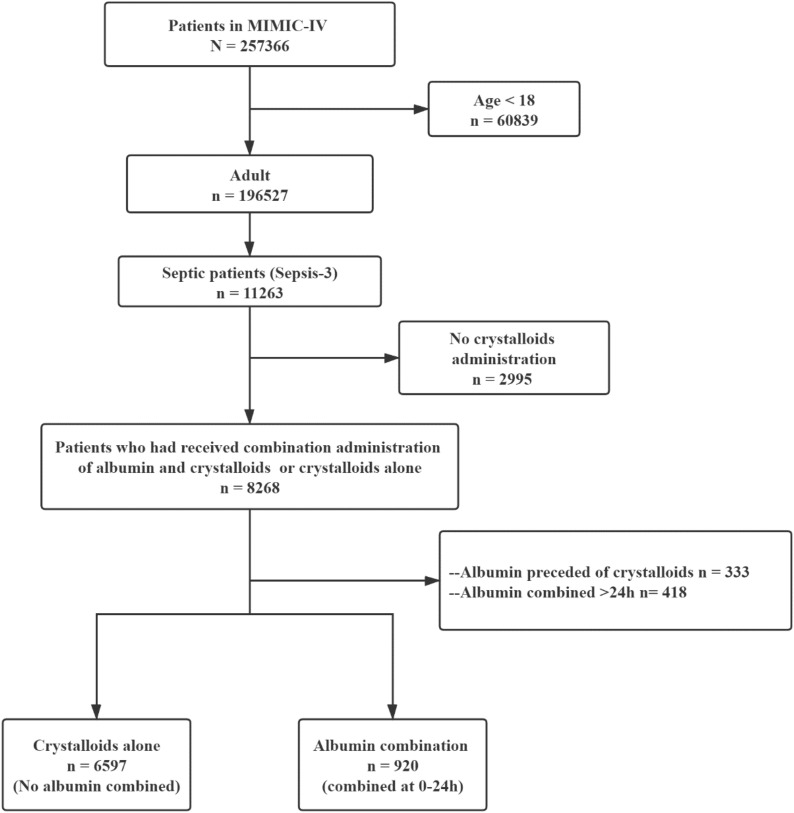
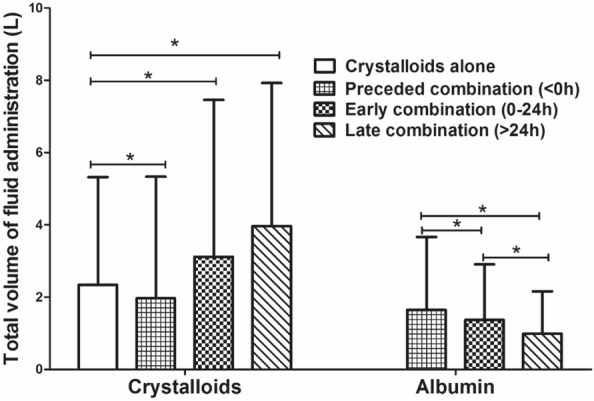
Methods: We involved septic patients from the Medical Information Mart for Intensive Care (MIMIC)-IV database, and these patients were categorized into crystalloids group (crystalloids alone) and early combination group (crystalloids combined albumin at 0-24 h). The primary outcome was 28-day mortality. We used propensity score matching (PSM) to adjust confounding and restricted mean survival time (RMST) analysis was conducted to quantify the beneficial effect on survival due to the combination group.
Results: We categorized 6597 and 920 patients in the "crystalloids alone" and "early combination", respectively. After PSM, compared to the crystalloids group, the combination group was associated with the increased survival among 28-day (increased survival: 3.39 days, 95% CI 2.53-4.25; P < 0.001) after ICU admission. Patients who received albumin combination at the first 24-h was associated with prolonged LOS in ICU (10.72 days vs. 8.24 days; P < 0.001) but lower risk of 28-day mortality (12.5% vs 16.4%, P = 0.003) than those received crystalloids alone.
Conclusion: In septic patients, receiving albumin combined within the first 24-h after crystalloids administration was associated with an increment of survival in 28 days.
Keywords: Albumins; Fluid therapy; Mortality; Restricted mean survival time; Sepsis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Early high-volume resuscitation with crystalloid solution combined with albumin improves survival of critically ill patients: A retrospective analysis from MIMIC-IV database.Burns. 2024 May;50(4):893-902. doi: 10.1016/j.burns.2024.01.016. Epub 2024 Jan 19. Burns. 2024. PMID: 38278752
-
Association between Initial Fluid Choice and Subsequent In-hospital Mortality during the Resuscitation of Adults with Septic Shock.Anesthesiology. 2015 Dec;123(6):1385-93. doi: 10.1097/ALN.0000000000000861. Anesthesiology. 2015. PMID: 26414499
-
Early Combination of Albumin With Crystalloid Administration Might Reduce Mortality in Patients With Cardiogenic Shock: An Over 10-Year Intensive Care Survey.Front Cardiovasc Med. 2022 May 27;9:879812. doi: 10.3389/fcvm.2022.879812. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35694666 Free PMC article.
-
Crystalloids vs. colloids for fluid resuscitation in the Intensive Care Unit: A systematic review and meta-analysis.J Crit Care. 2019 Apr;50:144-154. doi: 10.1016/j.jcrc.2018.11.031. Epub 2018 Nov 30. J Crit Care. 2019. PMID: 30540968
-
What is the Preferred Resuscitation Fluid for Patients with Severe Sepsis and Septic Shock?J Emerg Med. 2017 Dec;53(6):928-939. doi: 10.1016/j.jemermed.2017.08.093. Epub 2017 Oct 25. J Emerg Med. 2017. PMID: 29079487 Review.
Cited by
-
Impact on outcomes of measuring lactates prior to ICU in unselected heterogeneous critically ill patients: A propensity score analysis.PLoS One. 2022 Nov 28;17(11):e0277948. doi: 10.1371/journal.pone.0277948. eCollection 2022. PLoS One. 2022. PMID: 36441770 Free PMC article.
-
Thiamine supplementation may be associated with improved prognosis in patients with sepsis.Br J Nutr. 2023 Jul 28;130(2):239-248. doi: 10.1017/S0007114522003373. Epub 2022 Oct 19. Br J Nutr. 2023. PMID: 36259460 Free PMC article.
-
Infusion of Human Albumin on Acute Pancreatitis Therapy: New Tricks for Old Dog?Front Pharmacol. 2022 Jun 1;13:842108. doi: 10.3389/fphar.2022.842108. eCollection 2022. Front Pharmacol. 2022. PMID: 35721190 Free PMC article.
-
Acute kidney injury-attributable mortality in critically ill patients with sepsis.PeerJ. 2022 Mar 25;10:e13184. doi: 10.7717/peerj.13184. eCollection 2022. PeerJ. 2022. PMID: 35356476 Free PMC article.
-
Association between admission baseline blood potassium levels and all-cause mortality in patients with acute kidney injury combined with sepsis: A retrospective cohort study.PLoS One. 2024 Nov 20;19(11):e0309764. doi: 10.1371/journal.pone.0309764. eCollection 2024. PLoS One. 2024. PMID: 39565797 Free PMC article.
References
-
- Fleischmann C, Scherag A, Adhikari NKJ, Hartog CS, Tsaganos T, Schlattmann P, Angus DC, Reinhart K. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am J Respir Crit Care Med. 2016;193(3):259–272. doi: 10.1164/rccm.201504-0781OC. - DOI - PubMed
-
- Kadri SS, Rhee C, Strich JR, Morales MK, Hohmann S, Menchaca J, Suffredini AF, Danner RL, Klompas M. Estimating ten-year trends in septic shock incidence and mortality in United States academic medical centers using clinical data. Chest. 2017;151(2):278–285. doi: 10.1016/j.chest.2016.07.010. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
