

Predictors of Time-in-Range (70-180 mg/dL) Achieved Using a Closed-Loop Control System
- PMID: 33689454
- PMCID: PMC8252894
- DOI: 10.1089/dia.2020.0646
Predictors of Time-in-Range (70-180 mg/dL) Achieved Using a Closed-Loop Control System
Abstract
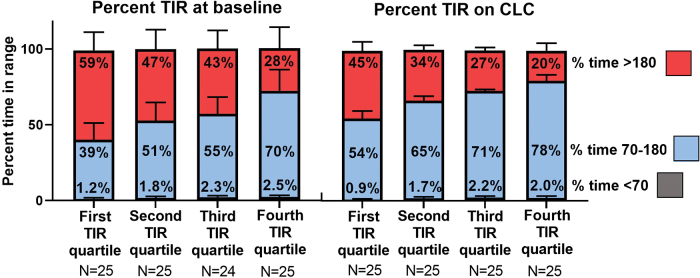
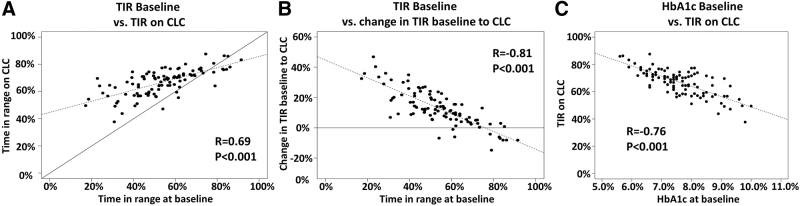
Background: Studies of closed-loop control (CLC) in patients with type 1 diabetes (T1D) consistently demonstrate improvements in glycemic control as measured by increased time-in-range (TIR) 70-180 mg/dL. However, clinical predictors of TIR in users of CLC systems are needed. Materials and Methods: We analyzed data from 100 children aged 6-13 years with T1D using the Tandem Control-IQ CLC system during a randomized trial or subsequent extension phase. Continuous glucose monitor data were collected at baseline and during 12-16 weeks of CLC use. Participants were stratified into quartiles of TIR on CLC to compare clinical characteristics. Results: TIR for those in the first, second, third, and fourth quartiles was 54%, 65%, 71%, and 78%, respectively. Lower baseline TIR was associated with lower TIR on CLC (r = 0.69, P < 0.001). However, lower baseline TIR was also associated with greater improvement in TIR on CLC (r = -0.81, P < 0.001). During CLC, participants in the highest versus lowest TIR-quartile administered more user-initiated boluses daily (8.5 ± 2.8 vs. 5.8 ± 2.6, P < 0.001) and received fewer automated boluses (3.5 ± 1.0 vs. 6.0 ± 1.6, P < 0.001). Participants in the lowest (vs. the highest) TIR-quartile received more insulin per body weight (1.13 ± 0.27 vs. 0.87 ± 0.20 U/kg/d, P = 0.008). However, in a multivariate model adjusting for baseline TIR, user-initiated boluses and insulin-per-body-weight were no longer significant. Conclusions: Higher baseline TIR is the strongest predictor of TIR on CLC in children with T1D. However, lower baseline TIR is associated with the greatest improvement in TIR. As with open-loop systems, user engagement is important for optimal glycemic control.
Keywords: Closed-loop systems; Insulin pump; Time-in-range; Type 1 diabetes.
Conflict of interest statement
M.J.S. received grant support, paid to her institution from Medtronic, Insulet and Tandem. L.G.K. has no disclosures to report. R.P.W. reports receiving grant support, consulting fees, and supplies, provided to his institution, from DexCom, advisory fees from Medtronic, and grant support, provided to his institution, from Tandem Diabetes Care and Bigfoot Biomedical, grant support, paid to his institution, advisory board fees, and supplies, provided to his institution, from Eli Lilly, and grant support, paid to his institution, and supplies, provided to his institution, from MannKind and Novo Nordisk. M.D.B. has no disclosures to report. K.J.R. has no disclosures to report. L.E. reports receiving consultancy fees from Tandem Diabetes Care. E.C. has no disclosures to report. E.J. has no disclosures to report. G.P.F. reports receiving grants support and lecture fees from Medtronic, MiniMed, Insulet, and Tandem, grant support from Abbott, and grant support and consulting fees from Eli Lilly. E.C.C. has no disclosures to report. L.H.M. has received speaking/consulting honoraria from Tandem Diabetes and DexCom, Inc., and also consults for Clinical Sensors and Capillary Biomedical; her institution receives research grants from Medtronic, Tandem Diabetes, DexCom, Abbott, and Insulet Corp. E.C. reports speaker and consultancy fees from Novo Nordisk, MannKind, Lexicon, and Arecor outside the submitted work. E.J. has no disclosures to report. L.C. has no disclosures to report. E.E. has no disclosures to report. L.J.H. has no disclosures to report. S.A.W. reports speaker and consultancy fees from Medtronic, Insulet, Zealand, and Sanofi outside the submitted work. B.A.B. reports receiving grant support and advisory board fees from Medtronic Diabetes and ConvaTec, grant support and presentation fees from Insulet, advisory board fees from Novo Nordisk and Profusa, grant support from Eli Lilly, grant support and equipment from DexCom, and holding patent 61197230 on a hypoglycemia prediction algorithm. R.A.L. has consulted for Abbott Diabetes Care, Biolinq, Capillary Biomedical, Morgan Stanley and Tidepool. M.O. has no disclosures to report. C.K. has no disclosures to report. B.B.D. has no disclosures to report. D.R.C. was a part time assistant professor of UVA at the time of the trial since then he transitioned to be a full-time employee of DexCom, Inc. R.W.B. reports receiving consulting fees, paid to his institution, from Insulet, Bigfoot Biomedical, and Eli Lilly, grant support and supplies, provided to his institution, from Tandem and DexCom, and supplies from Ascenia and Roche. M.D.D. received grant support, paid to his institution from Medtronic and Tandem.
Figures
References
-
- Levine BS, Anderson BJ, Butler DA, et al. : Predictors of glycemic control and short-term adverse outcomes in youth with type 1 diabetes. J Pediatr 2001;139:197–203 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
