

Pulmonary Embolism Does Not Have an Unusually High Incidence Among Hospitalized COVID19 Patients
- PMID: 33689493
- PMCID: PMC8718167
- DOI: 10.1177/1076029621996471
Pulmonary Embolism Does Not Have an Unusually High Incidence Among Hospitalized COVID19 Patients
Abstract
Introduction: Acute respiratory illnesses from COVID19 infection are increasing globally. Reports from earlier in the pandemic suggested that patients hospitalized for COVID19 are at particularly high risk for pulmonary embolism (PE). To estimate the incidences of PE during hospitalization for COVID19, we performed a rigorous systematic review of published literature.
Methods: We searched for case series, cohort studies and clinical trials from December 1, 2019 to July 13, 2020 that reported the incidence of PE among consecutive patients who were hospitalized for COVID19 in ICUs and in non-ICU hospital wards. To reflect the general population of hospitalized COVID19 patients, we excluded studies in which subject enrollment was linked to the clinical suspicion for venous thromboembolism (VTE).
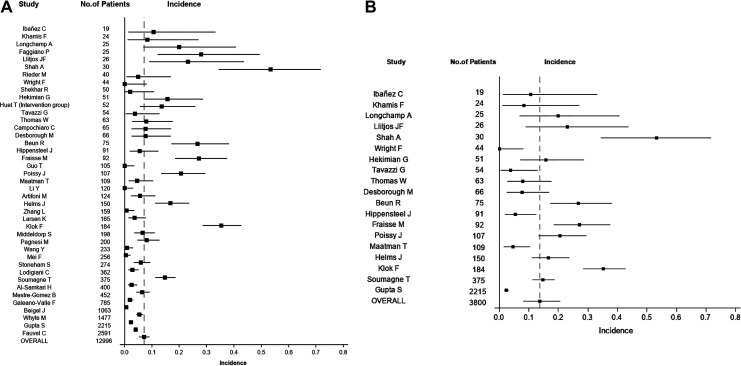
Results: Fifty-seven studies were included in the analysis. The combined random effects estimate of PE incidence among all hospitalized COVID19 patients was 7.1% (95% CI: 5.2%, 9.1%). Studies with larger sample sizes reported significantly lower PE incidences than smaller studies (r2 = 0.161, p = 0.036). The PE incidence among studies that included 400 or more patients was 3.0% (95% CI: 1.7%, 4.6%). Among COVID19 patients admitted to ICUs, the combined estimated PE incidence was 13.7% (95% CI: 8.0%, 20.6%). The incidence of ICU-related PE also decreased as the study sample sizes increased. The single largest COVID19 ICU study (n = 2215) disclosed a PE incidence of 2.3% (95% CI: 1.7%, 3.0%).
Conclusion: PE incidences among hospitalized COVID19 patients are much lower than has been previously postulated based on smaller, often biased study reports. The incidence of "microthrombosis," leading to occlusion of microscopic blood vessels, remains unknown.
Keywords: COVID-19; SARS-COV-2; deep venous thrombosis; pulmonary embolism; thromboembolism.
Conflict of interest statement
Figures


Similar articles
-
Deep vein thrombosis and pulmonary embolism among hospitalized coronavirus disease 2019-positive patients predicted for higher mortality and prolonged intensive care unit and hospital stays in a multisite healthcare system.J Vasc Surg Venous Lymphat Disord. 2021 Nov;9(6):1361-1370.e1. doi: 10.1016/j.jvsv.2021.03.009. Epub 2021 Apr 6. J Vasc Surg Venous Lymphat Disord. 2021. PMID: 33836287 Free PMC article.
-
The Incidence of Pulmonary Embolism in Hospitalized Non-ICU Patients with COVID-19 during the First Wave: A Multicenter Retrospective Cohort Study in the Netherlands.J Vasc Res. 2024;61(3):142-150. doi: 10.1159/000538312. Epub 2024 Apr 17. J Vasc Res. 2024. PMID: 38631294 Free PMC article.
-
Pulmonary Embolism in Hospitalized Patients with COVID-19: A Multicenter Study.Radiology. 2021 Dec;301(3):E426-E433. doi: 10.1148/radiol.2021210777. Epub 2021 Jul 13. Radiology. 2021. PMID: 34254850 Free PMC article.
-
A systematic review and meta-analysis of incidence, prognosis, and laboratory indicators of venous thromboembolism in hospitalized patients with coronavirus disease 2019.J Vasc Surg Venous Lymphat Disord. 2021 Sep;9(5):1099-1111.e6. doi: 10.1016/j.jvsv.2021.01.012. Epub 2021 Jan 30. J Vasc Surg Venous Lymphat Disord. 2021. PMID: 33529719 Free PMC article.
-
Incidence of acute pulmonary embolism in COVID-19 patients: Systematic review and meta-analysis.Eur J Intern Med. 2020 Dec;82:29-37. doi: 10.1016/j.ejim.2020.09.006. Epub 2020 Sep 17. Eur J Intern Med. 2020. PMID: 32958372 Free PMC article.
Cited by
-
A Prospective Study Evaluating Cumulative Incidence and a Specific Prediction Rule in Pulmonary Embolism in COVID-19.Front Med (Lausanne). 2022 Jul 1;9:936816. doi: 10.3389/fmed.2022.936816. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35847817 Free PMC article.
-
Prothrombotic State in COVID-19: Myth or Reality?Mayo Clin Proc. 2021 Jul;96(7):1694-1696. doi: 10.1016/j.mayocp.2021.05.015. Epub 2021 May 24. Mayo Clin Proc. 2021. PMID: 34218846 Free PMC article. No abstract available.
-
Supportive Care in Patients with Critical Coronavirus Disease 2019.Infect Dis Clin North Am. 2022 Dec;36(4):777-789. doi: 10.1016/j.idc.2022.08.003. Epub 2022 Aug 15. Infect Dis Clin North Am. 2022. PMID: 36328636 Free PMC article. Review.
-
Risk of Venous Thromboembolism in Infectious Diseases: A Literature Review.Pathogens. 2025 Aug 18;14(8):816. doi: 10.3390/pathogens14080816. Pathogens. 2025. PMID: 40872326 Free PMC article. Review.
-
Rebuttal From Dr David Jimenez et al.Chest. 2022 Jun;161(6):1453-1455. doi: 10.1016/j.chest.2022.01.038. Epub 2022 Mar 15. Chest. 2022. PMID: 35469672 Free PMC article. No abstract available.
References
-
- Song F, Parekh S, Hooper L, et al. Dissemination and publication of research findings: an updated review of related biases. Health Technol Assess. 2010;14(8):iii, ix–xi, 1–193. doi:10.3310/hta14080 - PubMed
-
- Easterbrook PJ, Berlin JA, Gopalan R, Matthews DR. Publication bias in clinical research. Lancet. 1991;337(8746):867–872. doi:10.1016/0140-6736(91)90201-y - PubMed
-
- Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–2012. - PubMed
-
- Clopper CJ, Pearson ES. The use of confidence or fiducial limits illustrated in the case of the binomial. Biometrika. 1934;26:404–413.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
