

SOCS-1 inhibition of type I interferon restrains Staphylococcus aureus skin host defense
- PMID: 33690673
- PMCID: PMC7984627
- DOI: 10.1371/journal.ppat.1009387
SOCS-1 inhibition of type I interferon restrains Staphylococcus aureus skin host defense
Abstract
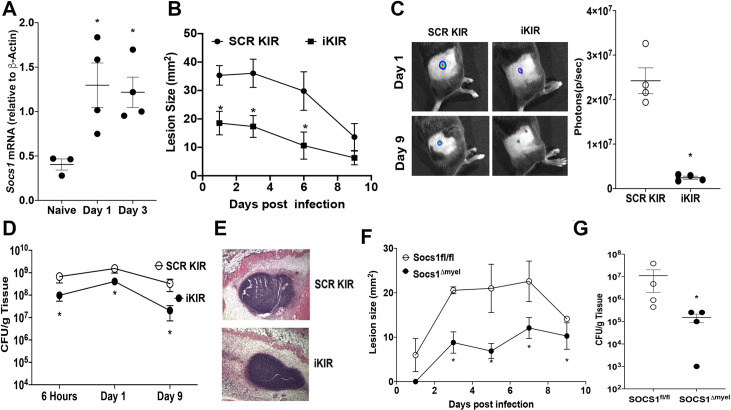
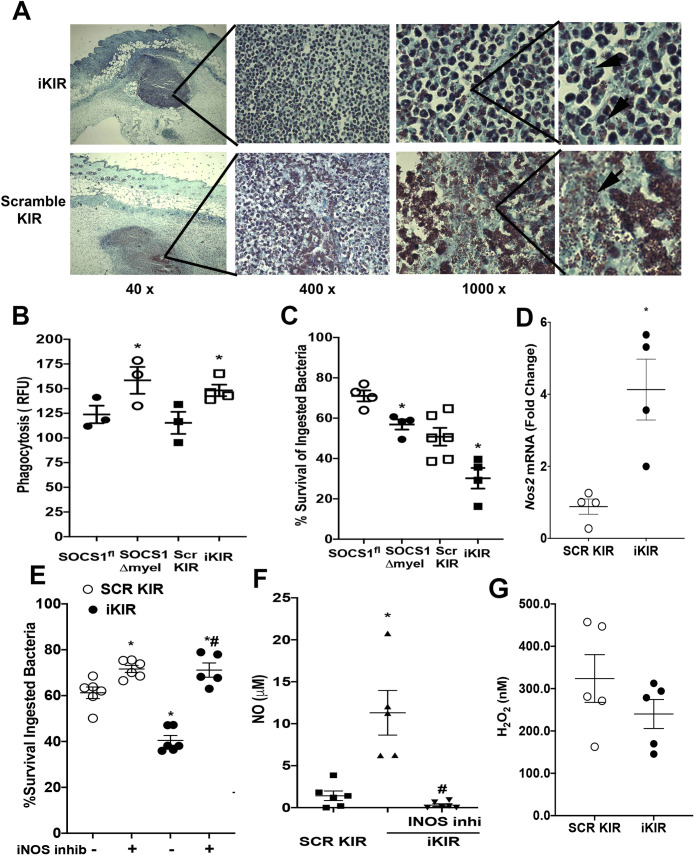
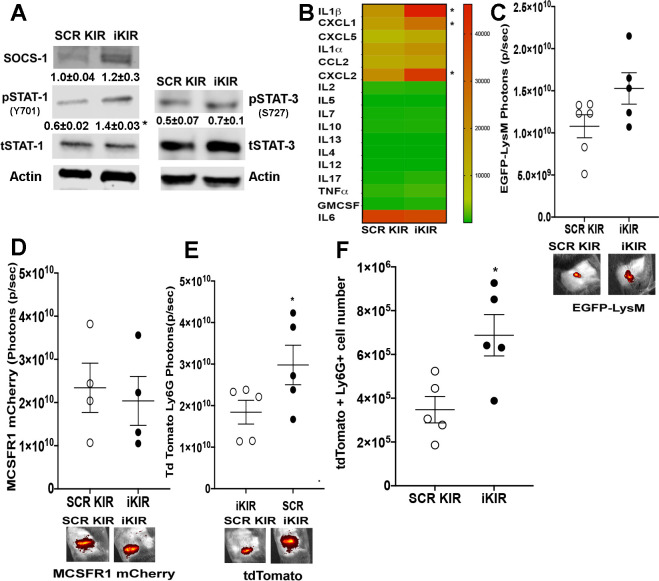
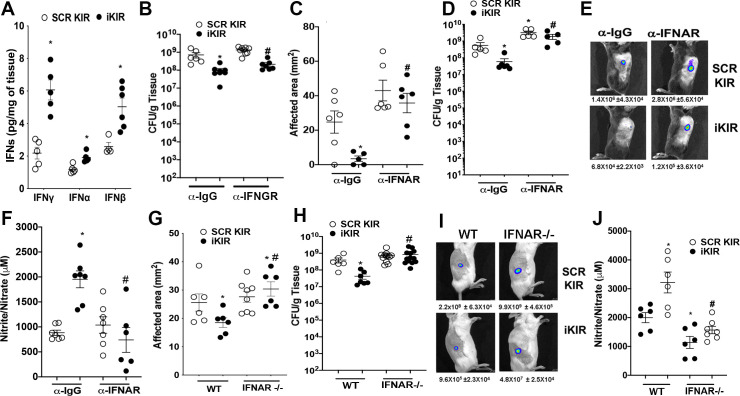
The skin innate immune response to methicillin-resistant Staphylococcus aureus (MRSA) culminates in the formation of an abscess to prevent bacterial spread and tissue damage. Pathogen recognition receptors (PRRs) dictate the balance between microbial control and injury. Therefore, intracellular brakes are of fundamental importance to tune the appropriate host defense while inducing resolution. The intracellular inhibitor suppressor of cytokine signaling 1 (SOCS-1), a known JAK/STAT inhibitor, prevents the expression and actions of PRR adaptors and downstream effectors. Whether SOCS-1 is a molecular component of skin host defense remains to be determined. We hypothesized that SOCS-1 decreases type I interferon production and IFNAR-mediated antimicrobial effector functions, limiting the inflammatory response during skin infection. Our data show that MRSA skin infection enhances SOCS-1 expression, and both SOCS-1 inhibitor peptide-treated and myeloid-specific SOCS-1 deficient mice display decreased lesion size, bacterial loads, and increased abscess thickness when compared to wild-type mice treated with the scrambled peptide control. SOCS-1 deletion/inhibition increases phagocytosis and bacterial killing, dependent on nitric oxide release. SOCS-1 inhibition also increases the levels of type I and type II interferon levels in vivo. IFNAR deletion and antibody blockage abolished the beneficial effects of SOCS-1 inhibition in vivo. Notably, we unveiled that hyperglycemia triggers aberrant SOCS-1 expression that correlates with decreased overall IFN signatures in the infected skin. SOCS-1 inhibition restores skin host defense in the highly susceptible hyperglycemic mice. Overall, these data demonstrate a role for SOCS-1-mediated type I interferon actions in host defense and inflammation during MRSA skin infection.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Edelsberg J, Taneja C, Zervos M, Haque N, Moore C, Reyes K, et al. Trends in US hospital admissions for skin and soft tissue infections. Emerg Infect Dis [Internet]. 2009. September [cited 2020 Apr 23];15(9):1516–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19788830 10.3201/eid1509.081228 - DOI - PMC - PubMed
-
- Watkins RR, Holubar M, David MZ. Antimicrobial Resistance in Methicillin-Resistant Staphylococcus aureus to Newer Antimicrobial Agents. Antimicrob Agents Chemother [Internet]. 2019. September 16 [cited 2020 Apr 23];63(12). Available from: http://www.ncbi.nlm.nih.gov/pubmed/31527033 10.1128/AAC.01216-19 - DOI - PMC - PubMed
-
- Cho JS, Guo Y, Ramos RI, Hebroni F, Plaisier SB. Neutrophil-derived IL-1b Is Sufficient for Abscess Formation in Immunity against Staphylococcus aureus in Mice. PLoS Pathog [Internet]. 2012. [cited 2020 Apr 14];8(11):1003047. Available from: www.plospathogens.org - PMC - PubMed
-
- Cheng AG, DeDent AC, Schneewind O, Missiakas D. A play in four acts: Staphylococcus aureus abscess formation [Internet]. Vol. 19, Trends in Microbiology. 2011. [cited 2020 Apr 30]. p. 225–32. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21353779 10.1016/j.tim.2011.01.007 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
