

Clinical prediction rule for SARS-CoV-2 infection from 116 U.S. emergency departments 2-22-2021
- PMID: 33690722
- PMCID: PMC7946184
- DOI: 10.1371/journal.pone.0248438
Clinical prediction rule for SARS-CoV-2 infection from 116 U.S. emergency departments 2-22-2021
Abstract
Objectives: Accurate and reliable criteria to rapidly estimate the probability of infection with the novel coronavirus-2 that causes the severe acute respiratory syndrome (SARS-CoV-2) and associated disease (COVID-19) remain an urgent unmet need, especially in emergency care. The objective was to derive and validate a clinical prediction score for SARS-CoV-2 infection that uses simple criteria widely available at the point of care.
Methods: Data came from the registry data from the national REgistry of suspected COVID-19 in EmeRgency care (RECOVER network) comprising 116 hospitals from 25 states in the US. Clinical variables and 30-day outcomes were abstracted from medical records of 19,850 emergency department (ED) patients tested for SARS-CoV-2. The criterion standard for diagnosis of SARS-CoV-2 required a positive molecular test from a swabbed sample or positive antibody testing within 30 days. The prediction score was derived from a 50% random sample (n = 9,925) using unadjusted analysis of 107 candidate variables as a screening step, followed by stepwise forward logistic regression on 72 variables.
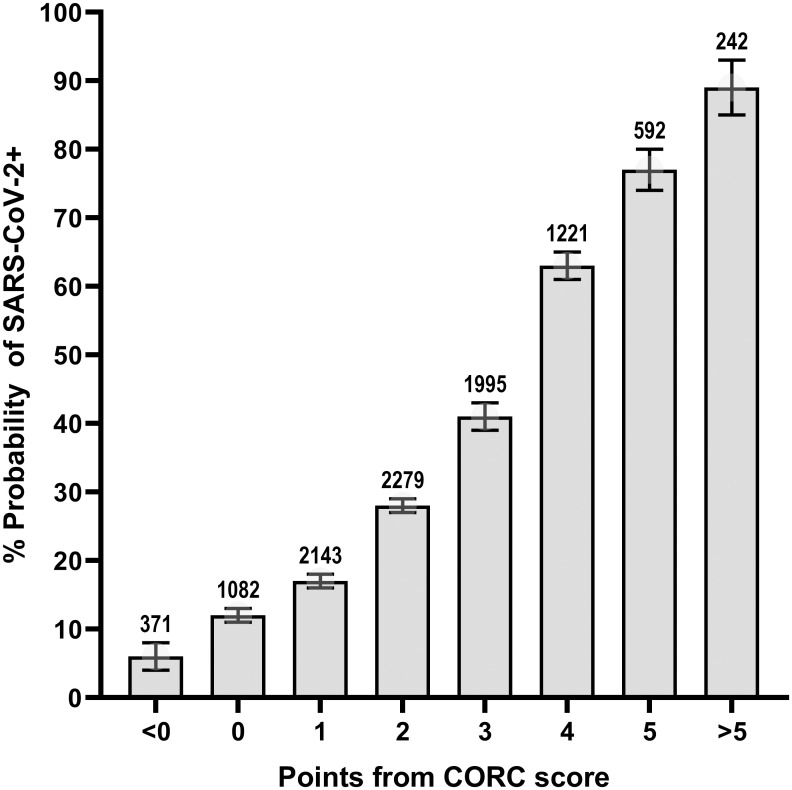
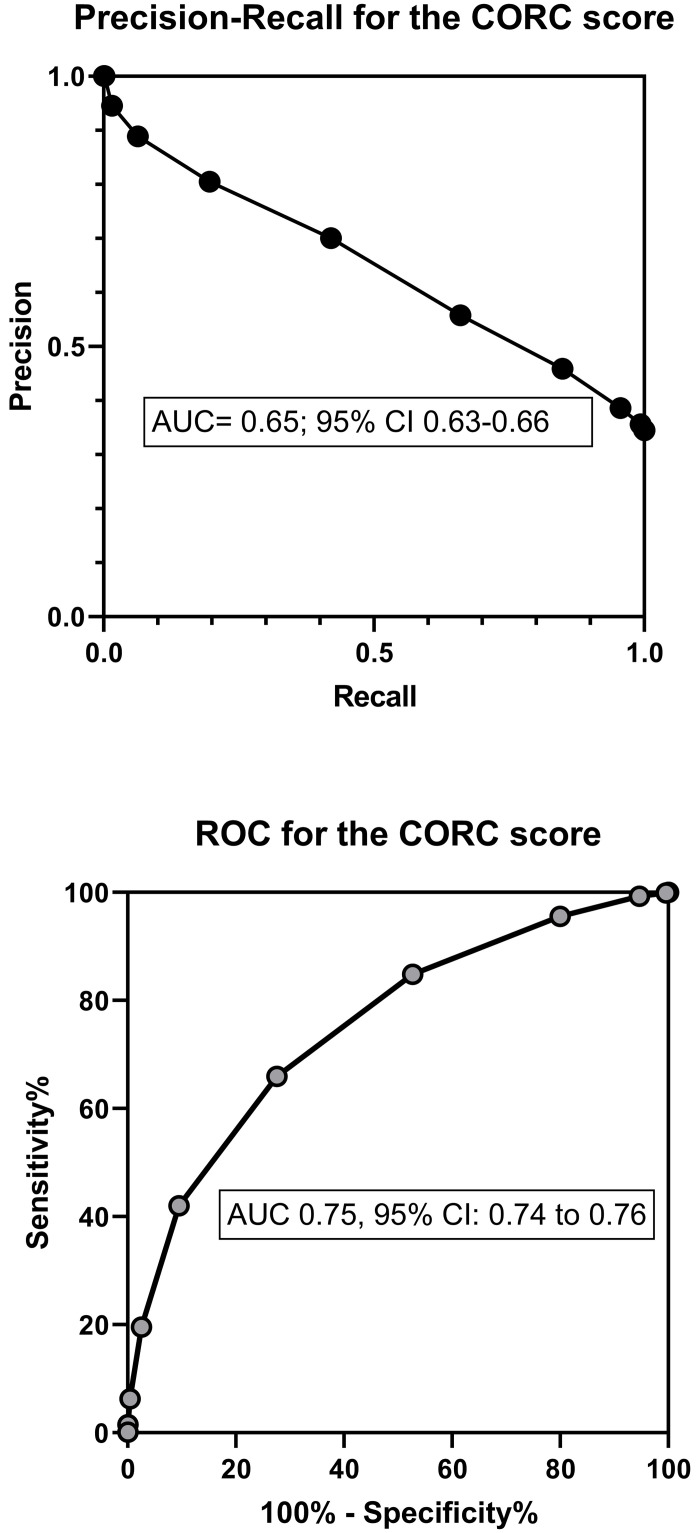
Results: Multivariable regression yielded a 13-variable score, which was simplified to a 13-point score: +1 point each for age>50 years, measured temperature>37.5°C, oxygen saturation<95%, Black race, Hispanic or Latino ethnicity, household contact with known or suspected COVID-19, patient reported history of dry cough, anosmia/dysgeusia, myalgias or fever; and -1 point each for White race, no direct contact with infected person, or smoking. In the validation sample (n = 9,975), the probability from logistic regression score produced an area under the receiver operating characteristic curve of 0.80 (95% CI: 0.79-0.81), and this level of accuracy was retained across patients enrolled from the early spring to summer of 2020. In the simplified score, a score of zero produced a sensitivity of 95.6% (94.8-96.3%), specificity of 20.0% (19.0-21.0%), negative likelihood ratio of 0.22 (0.19-0.26). Increasing points on the simplified score predicted higher probability of infection (e.g., >75% probability with +5 or more points).
Conclusion: Criteria that are available at the point of care can accurately predict the probability of SARS-CoV-2 infection. These criteria could assist with decisions about isolation and testing at high throughput checkpoints.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
