

Clinical prediction rule for SARS-CoV-2 infection from 116 U.S. emergency departments 2-22-2021
- PMID: 33690722
- PMCID: PMC7946184
- DOI: 10.1371/journal.pone.0248438
Clinical prediction rule for SARS-CoV-2 infection from 116 U.S. emergency departments 2-22-2021
Abstract
Objectives: Accurate and reliable criteria to rapidly estimate the probability of infection with the novel coronavirus-2 that causes the severe acute respiratory syndrome (SARS-CoV-2) and associated disease (COVID-19) remain an urgent unmet need, especially in emergency care. The objective was to derive and validate a clinical prediction score for SARS-CoV-2 infection that uses simple criteria widely available at the point of care.
Methods: Data came from the registry data from the national REgistry of suspected COVID-19 in EmeRgency care (RECOVER network) comprising 116 hospitals from 25 states in the US. Clinical variables and 30-day outcomes were abstracted from medical records of 19,850 emergency department (ED) patients tested for SARS-CoV-2. The criterion standard for diagnosis of SARS-CoV-2 required a positive molecular test from a swabbed sample or positive antibody testing within 30 days. The prediction score was derived from a 50% random sample (n = 9,925) using unadjusted analysis of 107 candidate variables as a screening step, followed by stepwise forward logistic regression on 72 variables.
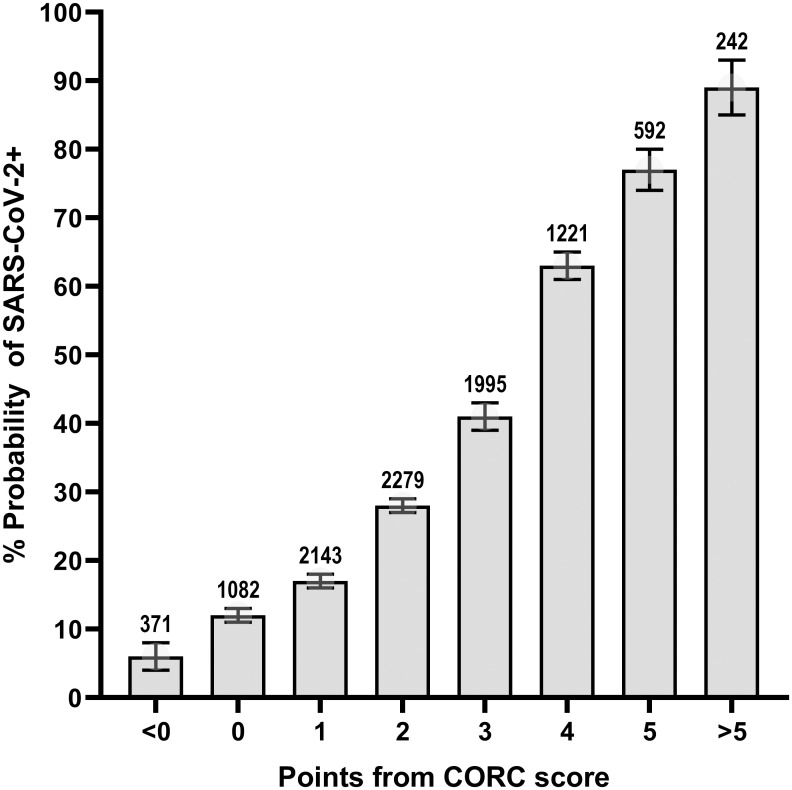
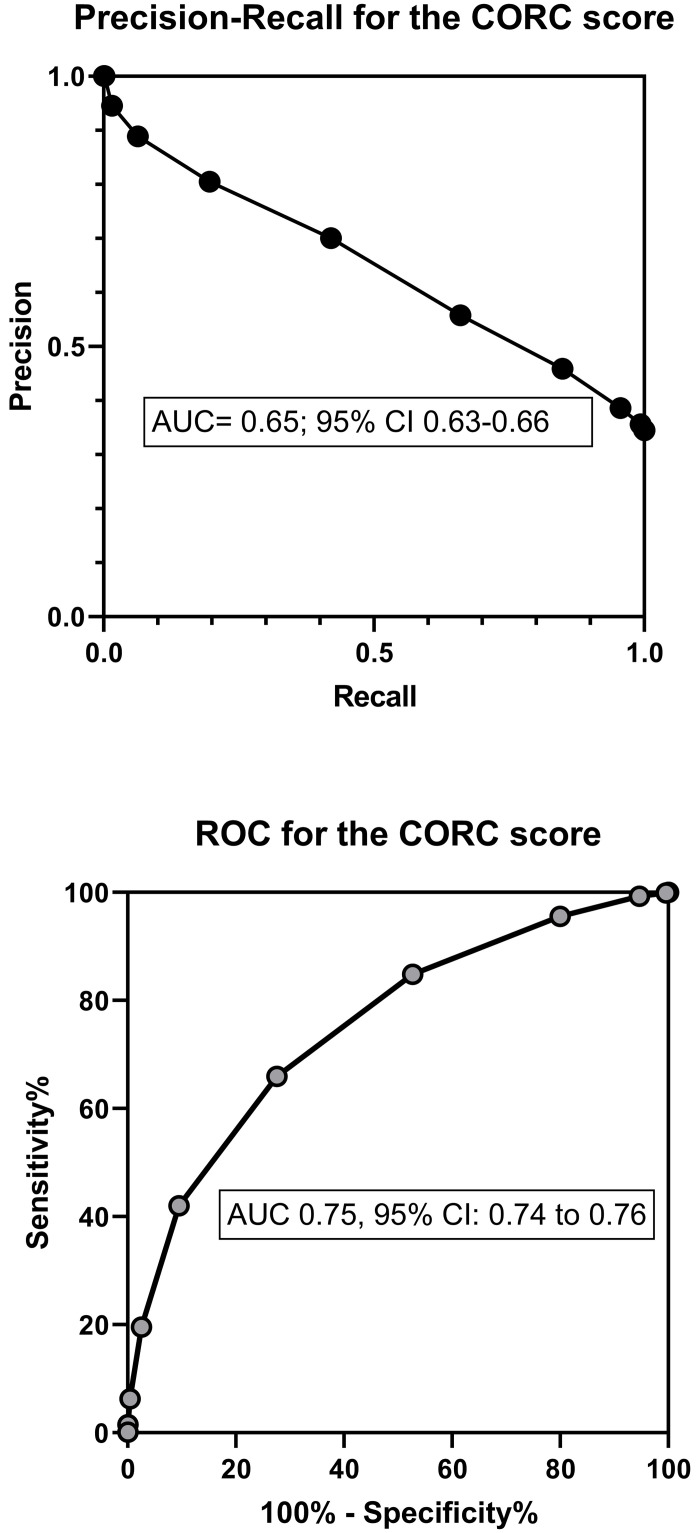
Results: Multivariable regression yielded a 13-variable score, which was simplified to a 13-point score: +1 point each for age>50 years, measured temperature>37.5°C, oxygen saturation<95%, Black race, Hispanic or Latino ethnicity, household contact with known or suspected COVID-19, patient reported history of dry cough, anosmia/dysgeusia, myalgias or fever; and -1 point each for White race, no direct contact with infected person, or smoking. In the validation sample (n = 9,975), the probability from logistic regression score produced an area under the receiver operating characteristic curve of 0.80 (95% CI: 0.79-0.81), and this level of accuracy was retained across patients enrolled from the early spring to summer of 2020. In the simplified score, a score of zero produced a sensitivity of 95.6% (94.8-96.3%), specificity of 20.0% (19.0-21.0%), negative likelihood ratio of 0.22 (0.19-0.26). Increasing points on the simplified score predicted higher probability of infection (e.g., >75% probability with +5 or more points).
Conclusion: Criteria that are available at the point of care can accurately predict the probability of SARS-CoV-2 infection. These criteria could assist with decisions about isolation and testing at high throughput checkpoints.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Which parameters support disposition decision in suspected COVID-19 cases in the emergency department (ED): a German clinical cohort study.BMJ Open. 2021 Mar 31;11(3):e044853. doi: 10.1136/bmjopen-2020-044853. BMJ Open. 2021. PMID: 33789854 Free PMC article.
-
Assessment of 135 794 Pediatric Patients Tested for Severe Acute Respiratory Syndrome Coronavirus 2 Across the United States.JAMA Pediatr. 2021 Feb 1;175(2):176-184. doi: 10.1001/jamapediatrics.2020.5052. JAMA Pediatr. 2021. PMID: 33226415 Free PMC article.
-
Clinical Prediction Tool to Assess the Likelihood of a Positive SARS-Cov-2 (COVID-19) Polymerase Chain Reaction Test in Patients with Flu-like Symptoms.West J Emerg Med. 2021 Mar 24;22(3):592-598. doi: 10.5811/westjem.2020.12.49200. West J Emerg Med. 2021. PMID: 34125032 Free PMC article.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
-
Diagnosis of COVID-19 in children guided by lack of fever and exposure to SARS-CoV-2.Pediatr Res. 2022 Apr;91(5):1196-1202. doi: 10.1038/s41390-021-01585-5. Epub 2021 Jun 11. Pediatr Res. 2022. PMID: 34117360 Free PMC article. Review.
Cited by
-
External validation of the 4C Mortality Score for hospitalised patients with COVID-19 in the RECOVER network.BMJ Open. 2022 Apr 21;12(4):e054700. doi: 10.1136/bmjopen-2021-054700. BMJ Open. 2022. PMID: 35450898 Free PMC article.
-
Age-related differences in symptoms in older emergency department patients with COVID-19: Prevalence and outcomes in a multicenter cohort.J Am Geriatr Soc. 2022 Jul;70(7):1918-1930. doi: 10.1111/jgs.17816. Epub 2022 Apr 29. J Am Geriatr Soc. 2022. PMID: 35460268 Free PMC article.
-
Process Improvement Approaches for Increasing the Response of Emergency Departments against the COVID-19 Pandemic: A Systematic Review.Int J Environ Res Public Health. 2021 Aug 20;18(16):8814. doi: 10.3390/ijerph18168814. Int J Environ Res Public Health. 2021. PMID: 34444561 Free PMC article.
-
Implementation of a COVID-19 screening tool in a southern Nigerian tertiary health facility.PLOS Glob Public Health. 2022 Aug 26;2(8):e0000578. doi: 10.1371/journal.pgph.0000578. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962763 Free PMC article.
-
Inter-rater reliability and prospective validation of a clinical prediction rule for SARS-CoV-2 infection.Acad Emerg Med. 2021 Jul;28(7):761-767. doi: 10.1111/acem.14309. Epub 2021 Jun 21. Acad Emerg Med. 2021. PMID: 34133794 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
