

Timing of surgery following SARS-CoV-2 infection: an international prospective cohort study
- PMID: 33690889
- PMCID: PMC8206995
- DOI: 10.1111/anae.15458
Timing of surgery following SARS-CoV-2 infection: an international prospective cohort study
Abstract
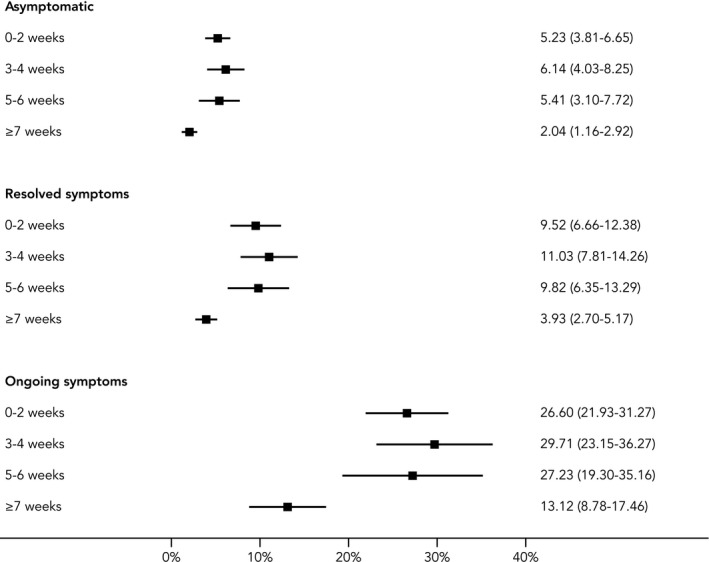
Peri-operative SARS-CoV-2 infection increases postoperative mortality. The aim of this study was to determine the optimal duration of planned delay before surgery in patients who have had SARS-CoV-2 infection. This international, multicentre, prospective cohort study included patients undergoing elective or emergency surgery during October 2020. Surgical patients with pre-operative SARS-CoV-2 infection were compared with those without previous SARS-CoV-2 infection. The primary outcome measure was 30-day postoperative mortality. Logistic regression models were used to calculate adjusted 30-day mortality rates stratified by time from diagnosis of SARS-CoV-2 infection to surgery. Among 140,231 patients (116 countries), 3127 patients (2.2%) had a pre-operative SARS-CoV-2 diagnosis. Adjusted 30-day mortality in patients without SARS-CoV-2 infection was 1.5% (95%CI 1.4-1.5). In patients with a pre-operative SARS-CoV-2 diagnosis, mortality was increased in patients having surgery within 0-2 weeks, 3-4 weeks and 5-6 weeks of the diagnosis (odds ratio (95%CI) 4.1 (3.3-4.8), 3.9 (2.6-5.1) and 3.6 (2.0-5.2), respectively). Surgery performed ≥ 7 weeks after SARS-CoV-2 diagnosis was associated with a similar mortality risk to baseline (odds ratio (95%CI) 1.5 (0.9-2.1)). After a ≥ 7 week delay in undertaking surgery following SARS-CoV-2 infection, patients with ongoing symptoms had a higher mortality than patients whose symptoms had resolved or who had been asymptomatic (6.0% (95%CI 3.2-8.7) vs. 2.4% (95%CI 1.4-3.4) vs. 1.3% (95%CI 0.6-2.0), respectively). Where possible, surgery should be delayed for at least 7 weeks following SARS-CoV-2 infection. Patients with ongoing symptoms ≥ 7 weeks from diagnosis may benefit from further delay.
주술기 SARS‐CoV‐2 감염은 수술 후 사망률을 증가시킨 다. 본 연구의 목적은 SARS‐CoV‐2에 감염된 환자에서 수술 전 계획된 지연(planned delay)의 최적 기간을 결정하는 것이 었다. 이 국제적 다기관 전향적 코호트 연구에는 2020년 10월 중에 정규 또는 응급 수술을 받은 환자가 포함되었다. 수술 전 SARS‐CoV‐2에 감염된 수술 대상 환자를 이전에 SARS‐ CoV‐2에 감염되지 않은 환자와 비교하였다. 일차 평가변수는 수술 후 30일 이내의 사망률이었다. 로지스틱 회귀분석 모델 을 사용하여 SARS‐CoV‐2 감염에서 수술까지의 경과 시간 에 따라 층화된 보정 30일 이내 사망률(adjusted 30‐day mortality rates)을 계산하였다. 14만 231명의 환자(116개국) 중 3127명(2.2%)이 수술 전에 SARS‐CoV‐2 감염 진단을 받았다. SARS‐CoV‐2에 감염되지 않은 환자의 보정 30일 이내 사망 률은 1.5%였다(95% 신뢰구간[CI] 1.4‐1.5). 수술 전 SARS‐CoV‐2 감염 진단을 받은 환자의 경우, 진단 후 0‐2주, 3‐4주 및 5‐6주 이내에 수술을 받은 환자에서 사망률이 증가하였다 (교차비[odds ratio] [95% CI]는 각각 4.1 [3.3‐4.8], 3.9 [2.6‐5.1] 및 3.6 [2.0‐5.2]). SARS‐CoV‐2 진단 후 7주 이상이 지난 뒤 실시된 수술은 기저치와 유사한 사망 위험도를 나타내었다 (교차비[95% CI] 1.5 [0.9‐2.1]). SARS‐CoV‐2에 감염된 뒤 7주 이상 수술이 연기된 경우, 증상이 지속된 환자는 증상이 관해되었거나 무증상인 환자보다 사망률이 더 높았다(각각 6.0% [95%CI 3.2‐8.7] 대비 2.4% [95%CI 1.4‐3.4] 대비 1.3% [95%CI 0.6‐2.0]). 가능하다면 SARS‐CoV‐2에 감염된 이후 최소 7주 동안 수술을 연기해야 한다. 진단 후 7주 이상 증상 이 지속되는 환자는 추가적인 수술 연기가 도움이 될 수 있다.
Keywords: COVID-19; SARS-CoV-2; delay; surgery; timing.
© 2021 The Authors. Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists.
Figures




Comment in
-
BMI- and age-related associations with mortality from COVID-19.Anaesthesia. 2022 Jan;77(1):107. doi: 10.1111/anae.15478. Epub 2021 Apr 11. Anaesthesia. 2022. PMID: 33840089 Free PMC article. No abstract available.
-
Effect of the COVID-19 pandemic on emergency gastrointestinal surgery in a university hospital in Paris over three consecutive years: A cohort study.Eur J Anaesthesiol. 2023 Jan 1;40(1):60-63. doi: 10.1097/EJA.0000000000001737. Eur J Anaesthesiol. 2023. PMID: 36479988 Free PMC article. No abstract available.
References
-
- Economist Intelligence Unit . Coronavirus vaccines: expect delays. Q1 global forecast 2021. 2021. https://www.eiu.com/n/campaigns/q1‐global‐forecast‐2021/ (accessed 01/02/2021).
Publication types
MeSH terms
Grants and funding
- Urology Foundation
- Vascular Society for Great Britain and Ireland
- NIHR Academy
- YCR_/Yorkshire Cancer Research/United Kingdom
- 211122/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- Bowel Disease Research Foundation
- British Association of Surgical Oncology
- Sarcoma UK
- DRF-2018-11-ST2-028/DH_/Department of Health/United Kingdom
- Bowel and Cancer Research
- Association of Upper Gastrointestinal Surgeons
- T32 DK060442/DK/NIDDK NIH HHS/United States
- Medtronic
- British Gynaecological Cancer Society
- K12 CA226330/CA/NCI NIH HHS/United States
- CH/17/1/32804/BHF_/British Heart Foundation/United Kingdom
- Association of Coloproctology of Great Britain and Ireland
- European Society of Coloproctology
- National Institute for Health Research (NIHR) Global Health Research Unit
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
