

A giant posterior mediastinal malignant peripheral nerve sheath tumor and benign neurofibroma in body surface: a case report
- PMID: 33691671
- PMCID: PMC7945373
- DOI: 10.1186/s12893-021-01122-5
A giant posterior mediastinal malignant peripheral nerve sheath tumor and benign neurofibroma in body surface: a case report
Abstract
Background: Neurofibromatosis comprises neurofibromatosis type 1 (NF1) and type 2 (NF2). Major tumor type of NF1 are neurofibroma recognized as benign peripheral nerve tumor, malignant peripheral nerve sheath tumor (MPNST), and glioma.
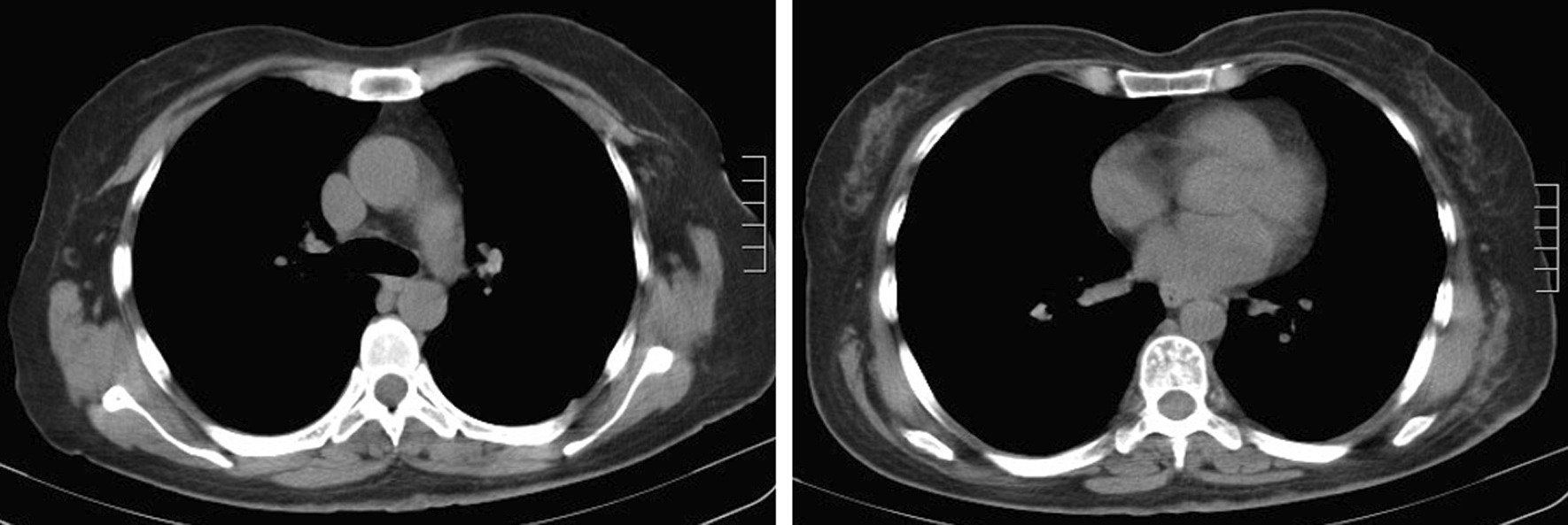
Case presentation: We report a woman with a special condition, whose tumors in body surfaces were benign neurofibroma and tumors in posterior mediastinum are MPNST. The chest-enhanced CT suggested a round soft tissue density in posteriormediastium. The diagnosis was established by pathology and immunohistochemistry. A single-stage thoracoscopic mediastinal mass resection was performed. The whole operation went smoothly and the CT scan of lungs did not show relapse of tumor three months later.
Conclusions: The appearance of neurofibroma should draw particular attention to the possibility of developing MPNST. More careful imaging examinations should be carried out, and pathological examination could diagnose it.
Keywords: Malignant peripheral nerve sheath tumor; Mediastinal tumor; Neurofibroma; Neurofibromatosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
