

The effects of clinical decision support system for prescribing medication on patient outcomes and physician practice performance: a systematic review and meta-analysis
- PMID: 33691690
- PMCID: PMC7944637
- DOI: 10.1186/s12911-020-01376-8
The effects of clinical decision support system for prescribing medication on patient outcomes and physician practice performance: a systematic review and meta-analysis
Abstract
Background: Clinical Decision Support Systems (CDSSs) for Prescribing are one of the innovations designed to improve physician practice performance and patient outcomes by reducing prescription errors. This study was therefore conducted to examine the effects of various CDSSs on physician practice performance and patient outcomes.
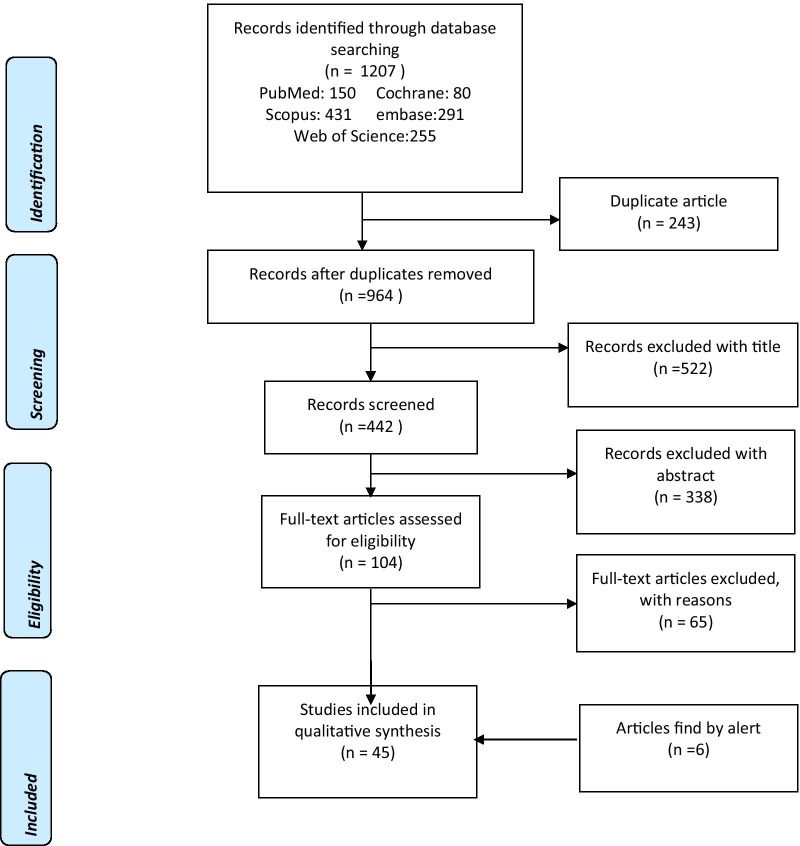
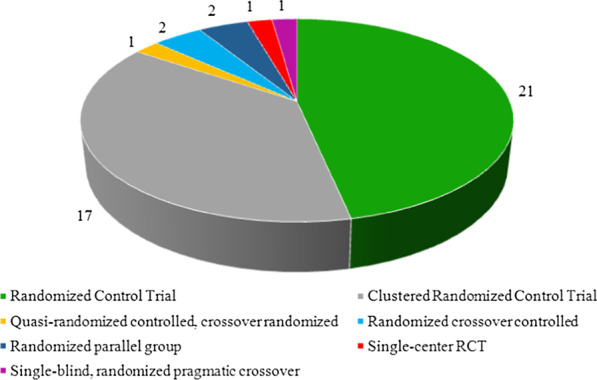
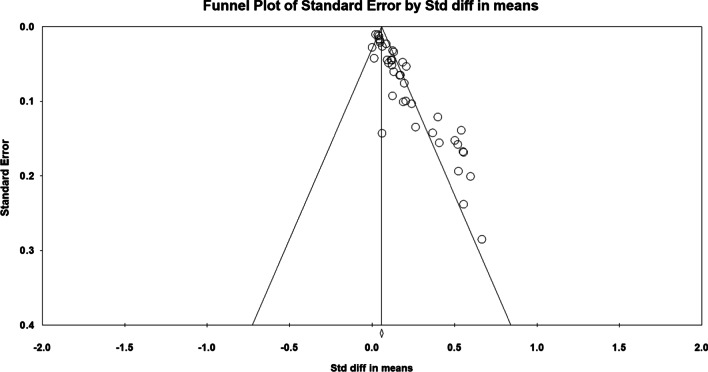
Methods: This systematic review was carried out by searching PubMed, Embase, Web of Science, Scopus, and Cochrane Library from 2005 to 2019. The studies were independently reviewed by two researchers. Any discrepancies in the eligibility of the studies between the two researchers were then resolved by consulting the third researcher. In the next step, we performed a meta-analysis based on medication subgroups, CDSS-type subgroups, and outcome categories. Also, we provided the narrative style of the findings. In the meantime, we used a random-effects model to estimate the effects of CDSS on patient outcomes and physician practice performance with a 95% confidence interval. Q statistics and I2 were then used to calculate heterogeneity.
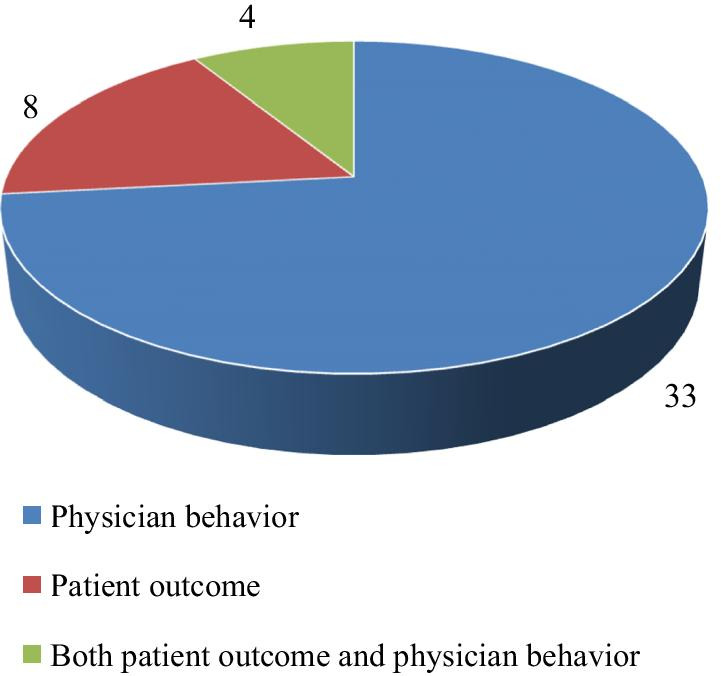
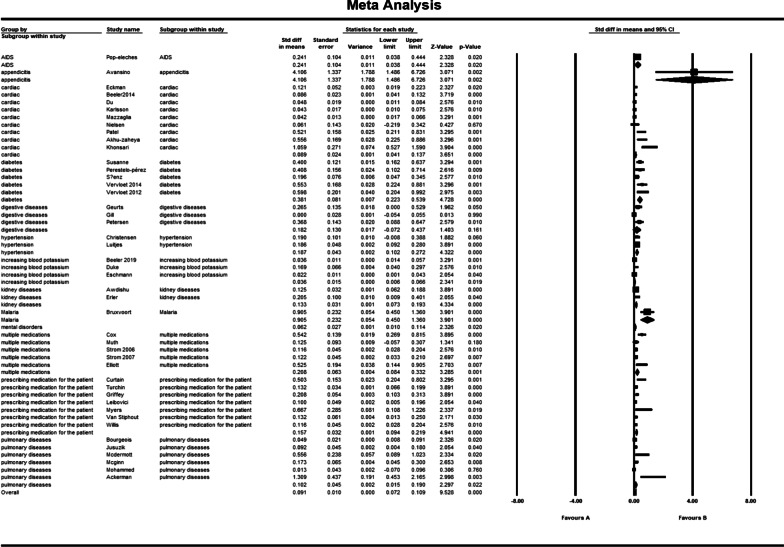
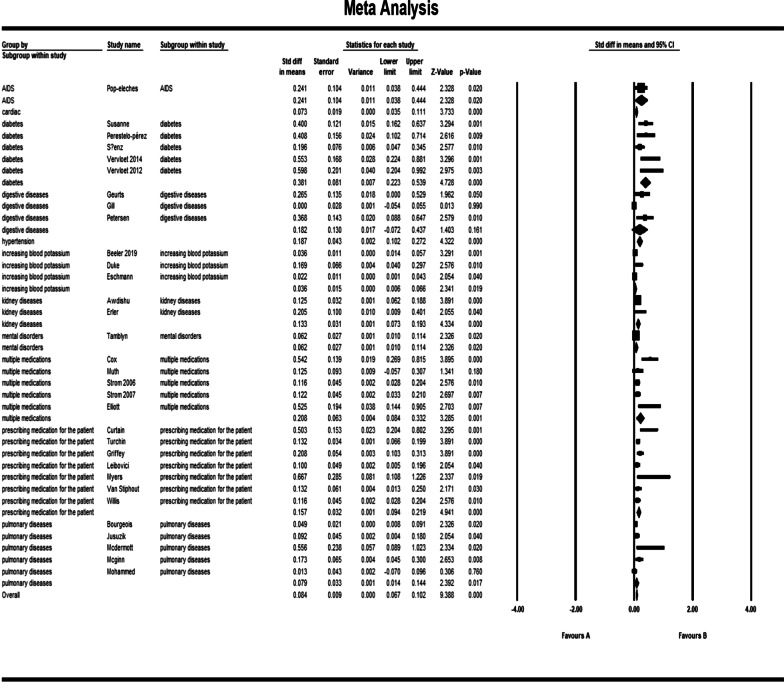
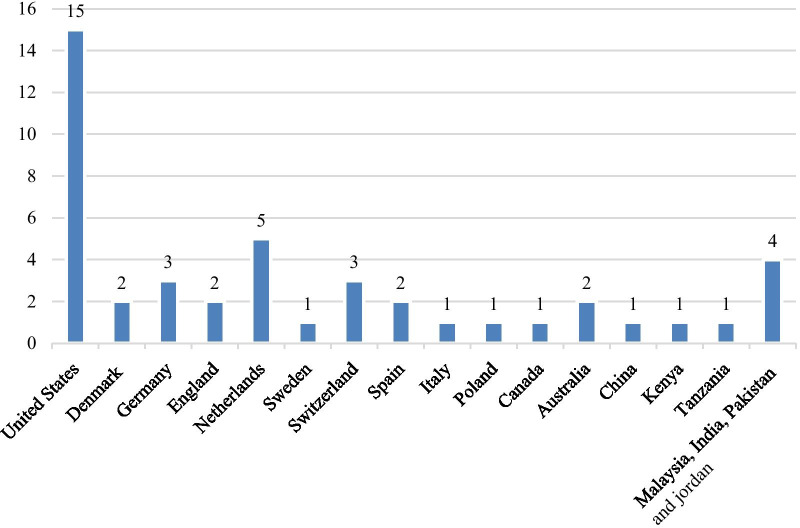
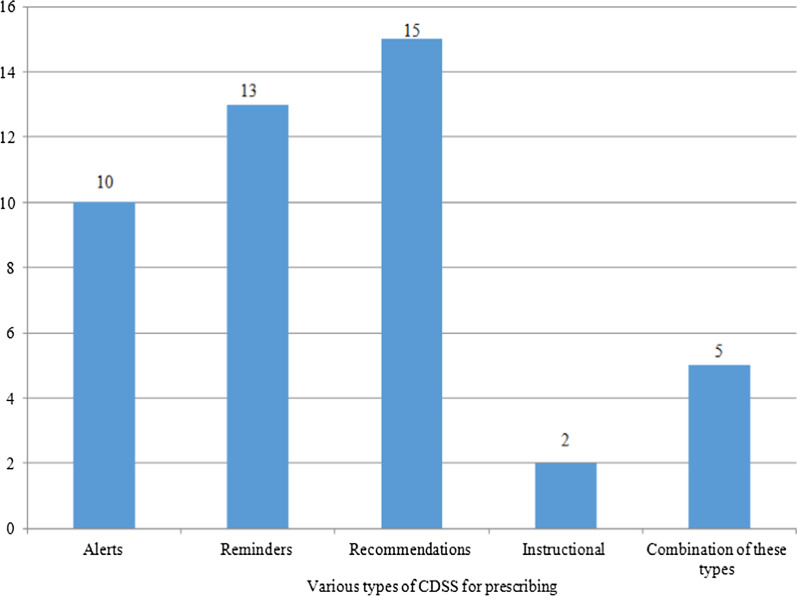
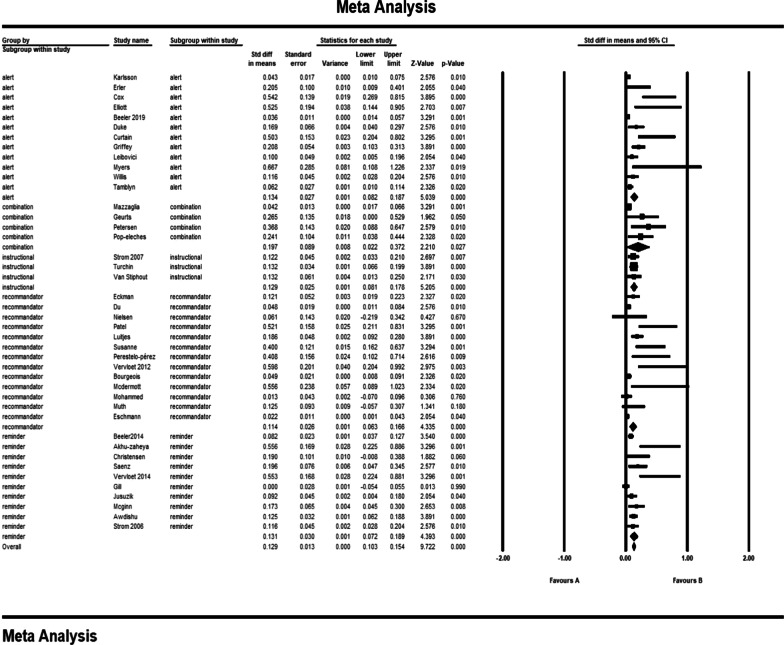
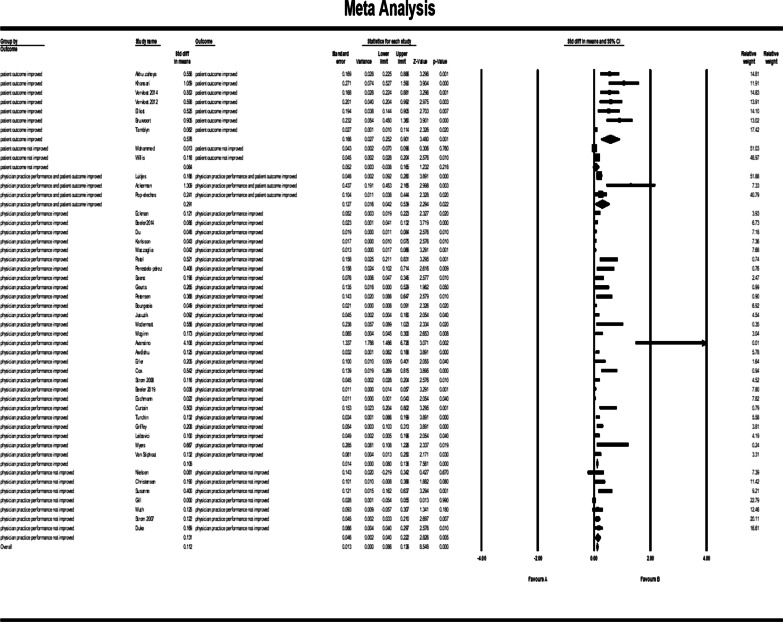
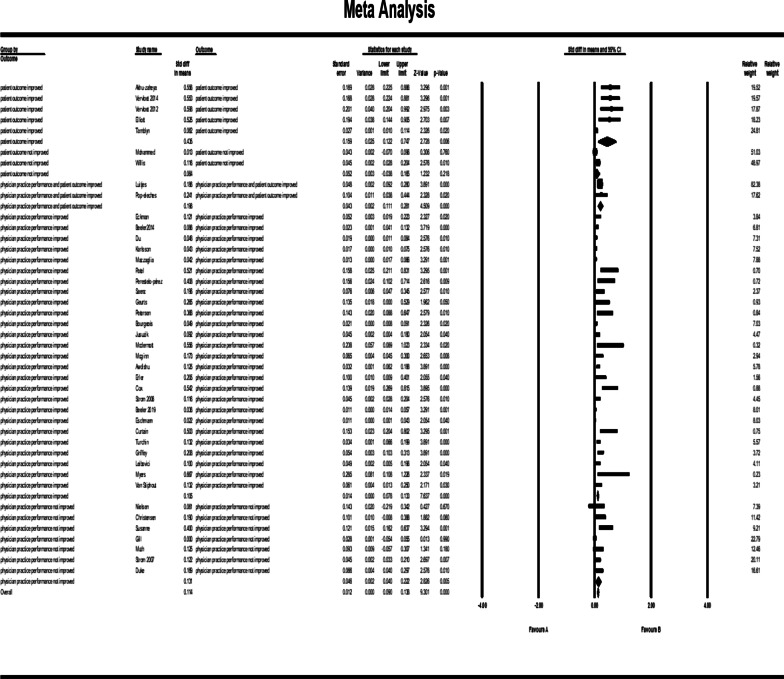
Results: On the basis of the inclusion criteria, 45 studies were qualified for analysis in this study. CDSS for prescription drugs/COPE has been used for various diseases such as cardiovascular diseases, hypertension, diabetes, gastrointestinal and respiratory diseases, AIDS, appendicitis, kidney disease, malaria, high blood potassium, and mental diseases. In the meantime, other cases such as concurrent prescribing of multiple medications for patients and their effects on the above-mentioned results have been analyzed. The study shows that in some cases the use of CDSS has beneficial effects on patient outcomes and physician practice performance (std diff in means = 0.084, 95% CI 0.067 to 0.102). It was also statistically significant for outcome categories such as those demonstrating better results for physician practice performance and patient outcomes or both. However, there was no significant difference between some other cases and traditional approaches. We assume that this may be due to the disease type, the quantity, and the type of CDSS criteria that affected the comparison. Overall, the results of this study show positive effects on performance for all forms of CDSSs.
Conclusions: Our results indicate that the positive effects of the CDSS can be due to factors such as user-friendliness, compliance with clinical guidelines, patient and physician cooperation, integration of electronic health records, CDSS, and pharmaceutical systems, consideration of the views of physicians in assessing the importance of CDSS alerts, and the real-time alerts in the prescription.
Keywords: Computerized clinical decision support systems; Medication prescription; Systematic review.
Conflict of interest statement
The authors declare that there are no financial and non-financial competing interests associated with this research.
Figures
References
-
- Moghaddasi H, Sheikhtaheri A, Hashemi N. Reducing medication errors: Role of computerized physician order entry system. J Health Adm. 2007;10(27):57–67.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
