

Ectopic sphenoid sinus pituitary adenoma masquerading as metastatic head and neck cancer
- PMID: 33692064
- PMCID: PMC7949438
- DOI: 10.1136/bcr-2020-240411
Ectopic sphenoid sinus pituitary adenoma masquerading as metastatic head and neck cancer
Abstract
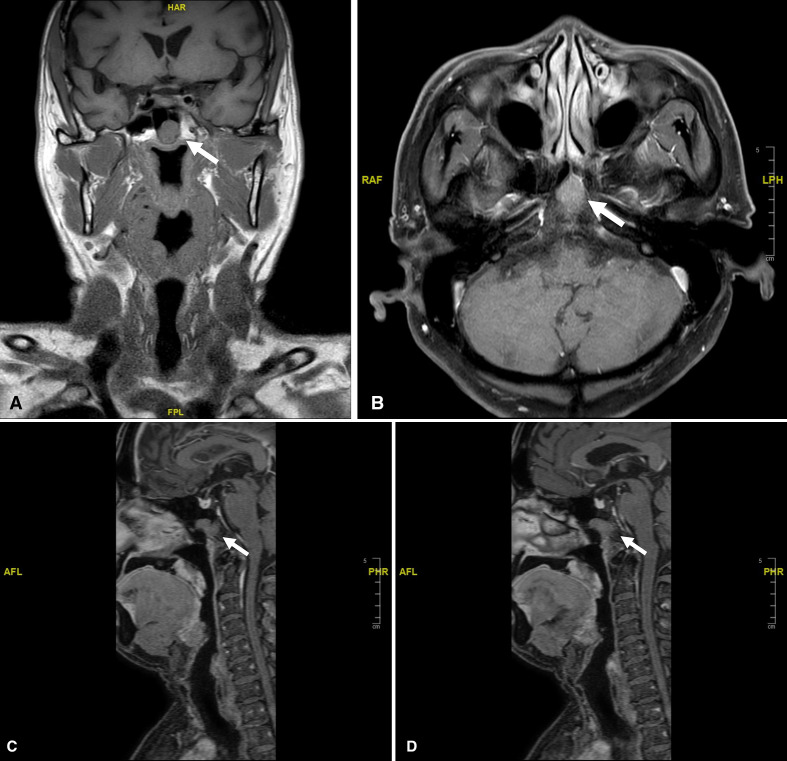
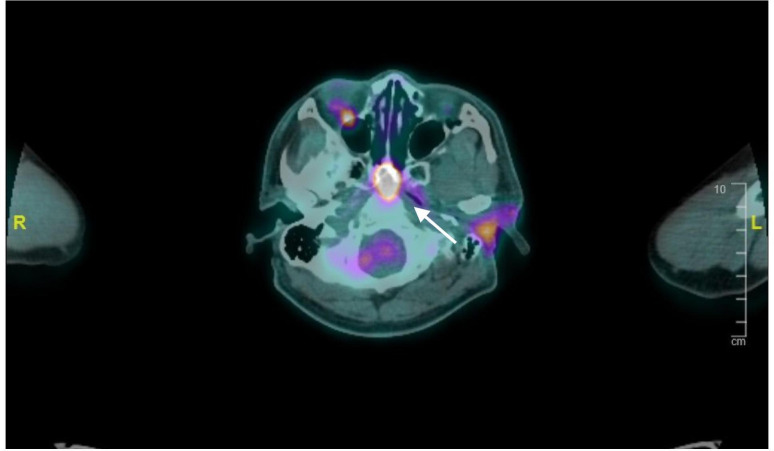
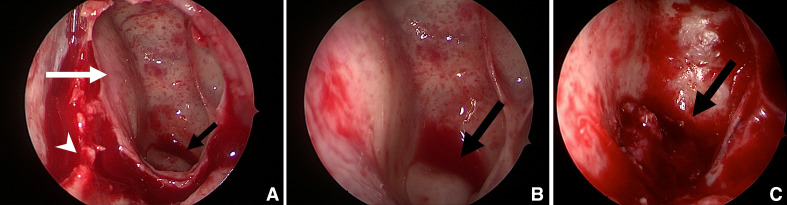
A 68-year-old Chinese man was found to have a lobular mass in the sphenoid sinus which extended to the clivus and the roof of the nasopharynx on a staging MRI scan performed for his high-grade parotid salivary duct carcinoma. Further positron emission tomography scan showed that this lesion was fluorodeoxyglucose (FDG) avid. This proved to be a diagnostic dilemma. The patient underwent a total parotidectomy, left selective neck dissection and a transphenoidal biopsy of his nasal lesion. Final histology revealed that this lesion was a synchronous ectopic sphenoid sinus pituitary adenoma (ESSPA). Initial differential diagnoses that were considered included a chordoma, metastatic carcinoma and nasopharyngeal carcinoma. However, an important differential with a neoplastic appearance and a tendency for positive FDG uptake is an ESSPA. It requires dedicated immunohistochemical staining to diagnose, and its mainstay of treatment is surgical excision.
Keywords: ear; head and neck cancer; neuroendocrinology; nose and throat/otolaryngology; radiology.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical