

Management of hospitalised adults with coronavirus disease 2019 (COVID-19): a European Respiratory Society living guideline
- PMID: 33692120
- PMCID: PMC7947358
- DOI: 10.1183/13993003.00048-2021
Management of hospitalised adults with coronavirus disease 2019 (COVID-19): a European Respiratory Society living guideline
Erratum in
-
"Management of hospitalised adults with coronavirus disease 2019 (COVID-19): a European Respiratory Society living guideline." James D. Chalmers, Megan L. Crichton, Pieter C. Goeminne, et al. Eur Respir J 2021; 57: 2100048.Eur Respir J. 2022 Aug 10;60(2):2150048. doi: 10.1183/13993003.50048-2021. Print 2022 Aug. Eur Respir J. 2022. PMID: 35948349 Free PMC article.
Abstract
Introduction: Hospitalised patients with coronavirus disease 2019 (COVID-19) as a result of SARS-CoV-2 infection have a high mortality rate and frequently require noninvasive respiratory support or invasive ventilation. Optimising and standardising management through evidence-based guidelines may improve quality of care and therefore patient outcomes.
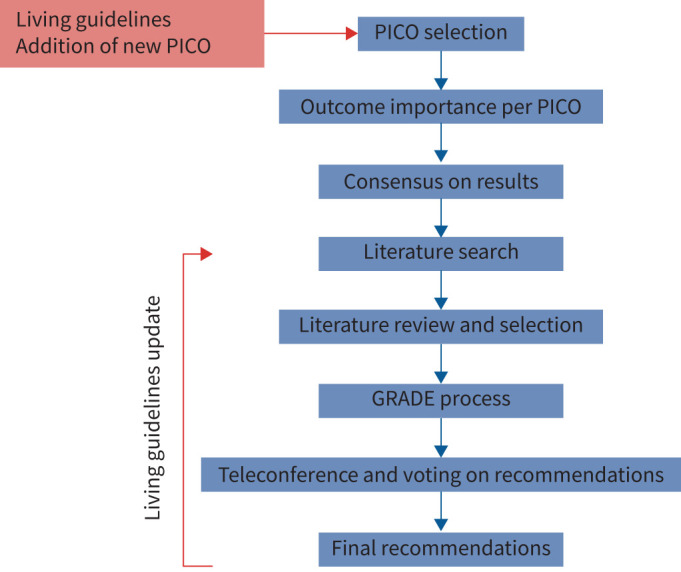
Methods: A task force from the European Respiratory Society and endorsed by the Chinese Thoracic Society identified priority interventions (pharmacological and non-pharmacological) for the initial version of this "living guideline" using the PICO (population, intervention, comparator, outcome) format. The GRADE approach was used for assessing the quality of evidence and strength of recommendations. Systematic literature reviews were performed, and data pooled by meta-analysis where possible. Evidence tables were presented and evidence to decision frameworks were used to formulate recommendations.
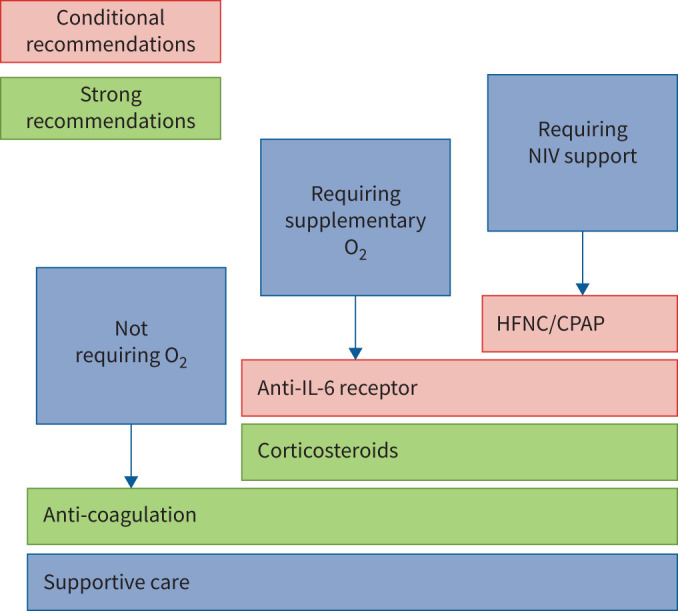
Results: Based on the available evidence at the time of guideline development (20 February, 2021), the panel makes a strong recommendation in favour of the use of systemic corticosteroids in patients requiring supplementary oxygen or ventilatory support, and for the use of anticoagulation in hospitalised patients. The panel makes a conditional recommendation for interleukin (IL)-6 receptor antagonist monoclonal antibody treatment and high-flow nasal oxygen or continuous positive airway pressure in patients with hypoxaemic respiratory failure. The panel make strong recommendations against the use of hydroxychloroquine and lopinavir-ritonavir. Conditional recommendations are made against the use of azithromycin, hydroxychloroquine combined with azithromycin, colchicine, and remdesivir, in the latter case specifically in patients requiring invasive mechanical ventilation. No recommendation was made for remdesivir in patients requiring supplemental oxygen. Further recommendations for research are made.
Conclusion: The evidence base for management of COVID-19 now supports strong recommendations in favour and against specific interventions. These guidelines will be regularly updated as further evidence becomes available.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: J.D. Chalmers reports grants and personal fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline and Insmed, grants from Gilead Sciences, personal fees from Chiesi, Novartis and Zambon, outside the submitted work. Conflict of interest: M.L. Crichton reports personal fees from AstraZeneca, outside the submitted work. Conflict of interest: P.C. Goeminne reports personal fees for lectures from GSK and AstraZeneca, grants, personal fees for advisory board work and non-financial support for meeting attendance from Chiesi, outside the submitted work. Conflict of interest: B. Cao reports personal fees from F. Hoffmann-La Roche Ltd as a member of a steering committee, and grants from Peking Union Medical College Foundation, outside the submitted work. Conflict of interest: M. Humbert reports grants, personal fees and non-financial support from GlaxoSmithKline, personal fees from AstraZeneca, Novartis, Roche, Sanofi, Teva and Merck, grants and personal fees from Acceleron, Actelion and Bayer, outside the submitted work. Conflict of interest: M. Shteinberg reports grants, personal fees and non-financial support from GSK, grants and personal fees from Novartis, personal fees from Boehringer Ingelheim, AstraZeneca, Kamada, Vertex Pharmaceuticals, Teva and Zambon, non-financial support from Actelion and Rafa, outside the submitted work. Conflict of interest: K.M. Antoniou has nothing to disclose. Conflict of interest: C.S. Ulrik reports grants from Mundipharma, personal fees from AstraZeneca, GSK, Chiesi, Orion Pharma and TEVA, grants and personal fees from Boehringer Ingelheim, Sanofi Genzyme and Novartis, outside the submitted work. Conflict of interest: H. Parks has nothing to disclose. Conflict of interest: C. Wang has nothing to disclose. Conflict of interest: T. Vandendriessche has nothing to disclose. Conflict of interest: J. Qu has nothing to disclose. Conflict of interest: D. Stolz reports grants from AstraZeneca AG, Curetis AG and Boston Scientific, lecture fees from AstraZeneca AG, Novartis AG, GSK AG, Roche AG, Zambon, Pfizer, Schwabe Pharma AG and Vifor AG, outside the submitted work. Conflict of interest: C. Brightling has nothing to disclose. Conflict of interest: T. Welte reports grants from German Ministry of Health, German Ministry of Research and Education, DFG, WHO and EU, during the conduct of the study; personal fees for lectures and advisory board work from Roche, AstraZeneca, Boehringer, GSK and Novartis, outside the submitted work. Conflict of interest: S. Aliberti reports grants and personal fees for advisory board work from Bayer Healthcare, personal fees for lectures from Grifols and Menarini, personal fees for advisory board work from AstraZeneca and ZetaCube Srl, personal fees for advisory board work and lectures from Zambon and GlaxoSmithKline, grants and personal fees for advisory board work and lectures from Chiesi and INSMED, grants from Fisher & Paykel, outside the submitted work. Conflict of interest: A.K. Simonds has nothing to disclose. Conflict of interest: T. Tonia acts as ERS methodologist. Conflict of interest: N. Roche reports grants and personal fees from Boehringer Ingelheim, Novartis and Pfizer, personal fees from GSK, AstraZeneca, Chiesi, Sanofi and Zambon, outside the submitted work.
Figures
Comment in
-
Guideline-directed management of COVID-19: Do's and Don'ts.Eur Respir J. 2021 Apr 15;57(4):2100753. doi: 10.1183/13993003.00753-2021. Print 2021 Apr. Eur Respir J. 2021. PMID: 33766949 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous