

Neutralization of SARS-CoV-2 with IgG from COVID-19-convalescent plasma
- PMID: 33692457
- PMCID: PMC7946899
- DOI: 10.1038/s41598-021-84733-5
Neutralization of SARS-CoV-2 with IgG from COVID-19-convalescent plasma
Abstract
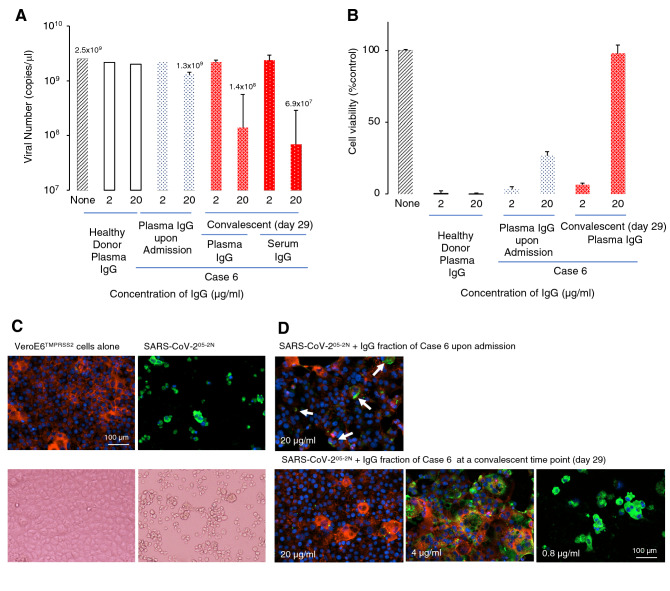
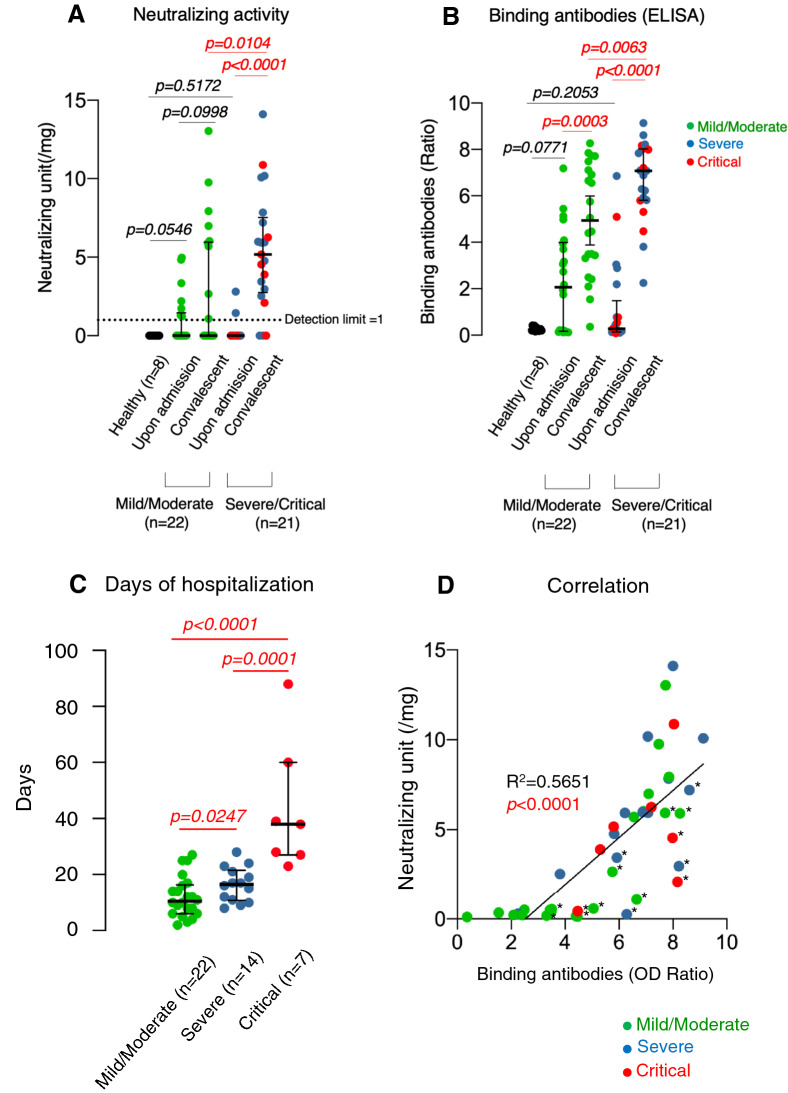
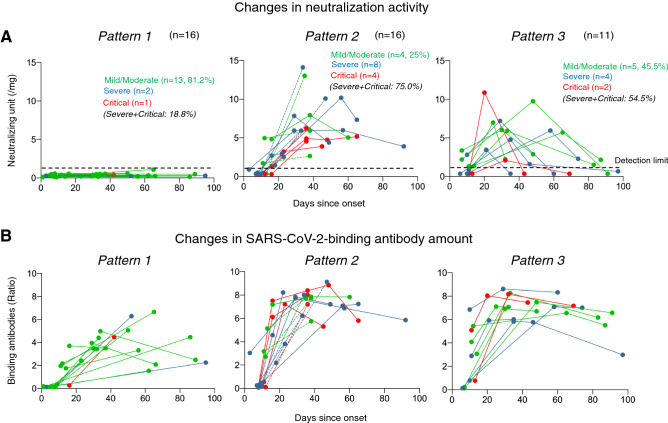
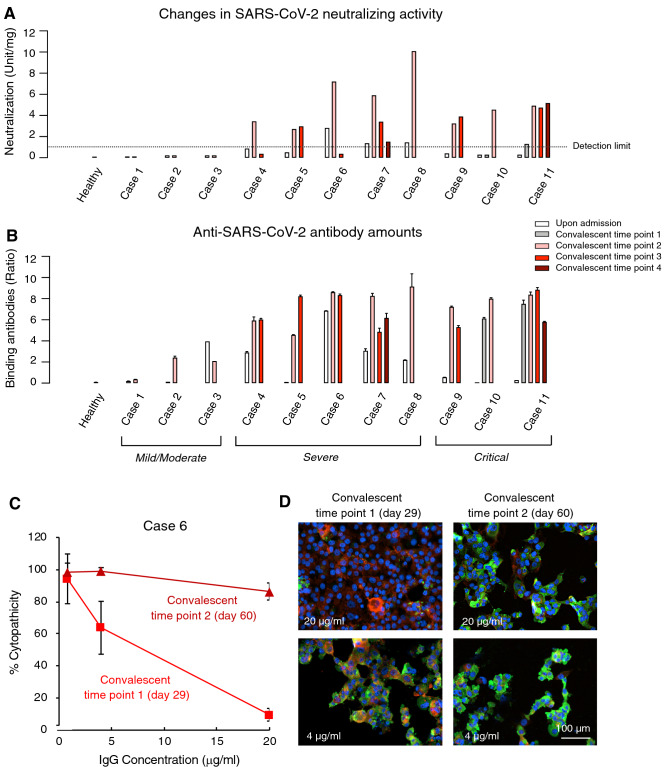
While there are various attempts to administer COVID-19-convalescent plasmas to SARS-CoV-2-infected patients, neither appropriate approach nor clinical utility has been established. We examined the presence and temporal changes of the neutralizing activity of IgG fractions from 43 COVID-19-convalescent plasmas using cell-based assays with multiple endpoints. IgG fractions from 27 cases (62.8%) had significant neutralizing activity and moderately to potently inhibited SARS-CoV-2 infection in cell-based assays; however, no detectable neutralizing activity was found in 16 cases (37.2%). Approximately half of the patients (~ 41%), who had significant neutralizing activity, lost the neutralization activity within ~ 1 month. Despite the rapid decline of neutralizing activity in plasmas, good amounts of SARS-CoV-2-S1-binding antibodies were persistently seen. The longer exposure of COVID-19 patients to greater amounts of SARS-CoV-2 elicits potent immune response to SARS-CoV-2, producing greater neutralization activity and SARS-CoV-2-S1-binding antibody amounts. The dilution of highly-neutralizing plasmas with poorly-neutralizing plasmas relatively readily reduced neutralizing activity. The presence of good amounts of SARS-CoV-2-S1-binding antibodies does not serve as a surrogate ensuring the presence of good neutralizing activity. In selecting good COVID-19-convalescent plasmas, quantification of neutralizing activity in each plasma sample before collection and use is required.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Dynamics of anti-SARS-CoV-2 antibodies in repeat convalescent plasma donors.Transfus Apher Sci. 2021 Dec;60(6):103216. doi: 10.1016/j.transci.2021.103216. Epub 2021 Jul 22. Transfus Apher Sci. 2021. PMID: 34315677 Free PMC article. No abstract available.
References
-
- World Health Organization. Coronavirus disease (COVID-19) outbreak situation. https://www.who.int/emergencies/diseases/novel-coronavirus-2019. (2020).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
