

COVID-19 and liver disease: mechanistic and clinical perspectives
- PMID: 33692570
- PMCID: PMC7945972
- DOI: 10.1038/s41575-021-00426-4
COVID-19 and liver disease: mechanistic and clinical perspectives
Abstract
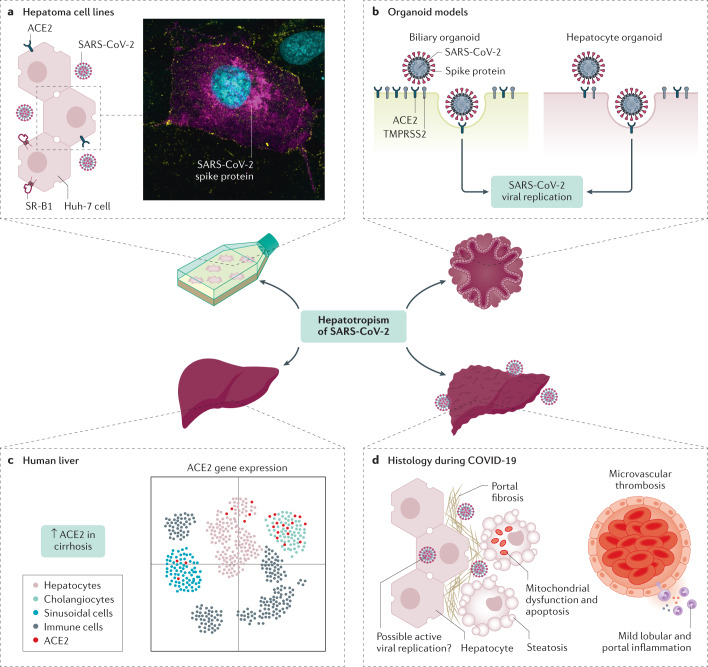
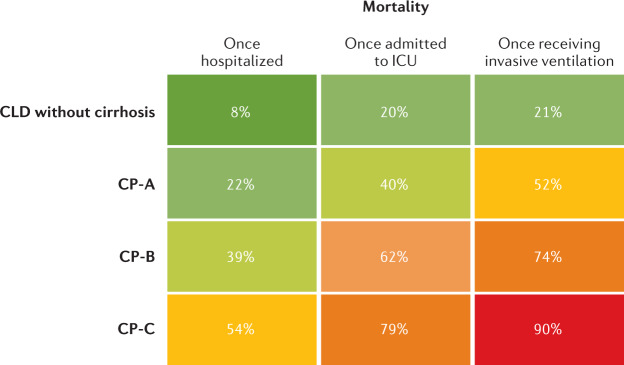
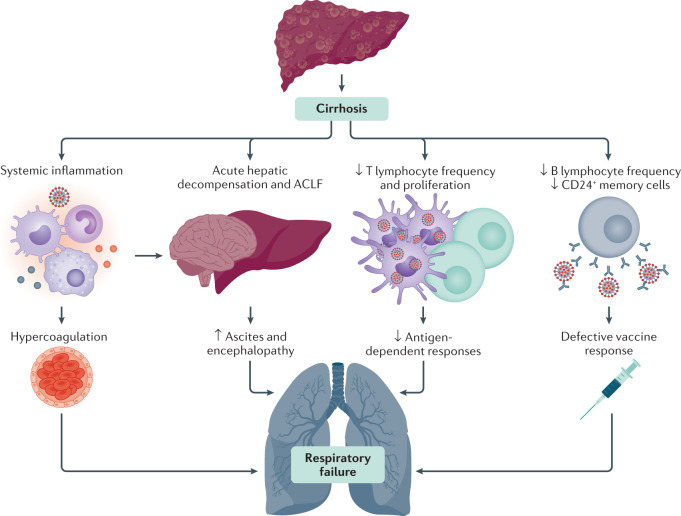
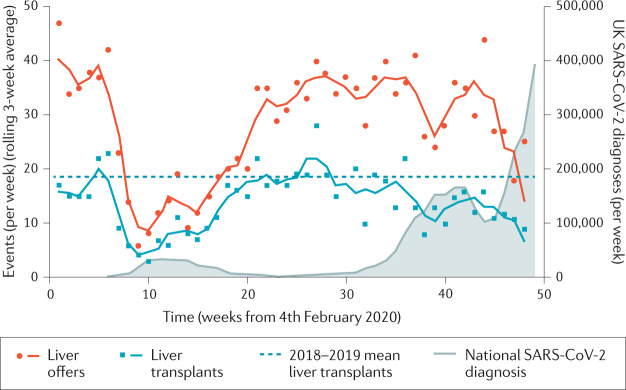
Our understanding of the hepatic consequences of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and its resultant coronavirus disease 2019 (COVID-19) has evolved rapidly since the onset of the pandemic. In this Review, we discuss the hepatotropism of SARS-CoV-2, including the differential expression of viral receptors on liver cell types, and we describe the liver histology features present in patients with COVID-19. We also provide an overview of the pattern and relevance of abnormal liver biochemistry during COVID-19 and present the possible underlying direct and indirect mechanisms for liver injury. Furthermore, large international cohorts have been able to characterize the disease course of COVID-19 in patients with pre-existing chronic liver disease. Patients with cirrhosis have particularly high rates of hepatic decompensation and death following SARS-CoV-2 infection and we outline hypotheses to explain these findings, including the possible role of cirrhosis-associated immune dysfunction. This finding contrasts with outcome data in pharmacologically immunosuppressed patients after liver transplantation who seem to have comparatively better outcomes from COVID-19 than those with advanced liver disease. Finally, we discuss the approach to SARS-CoV-2 vaccination in patients with cirrhosis and after liver transplantation and predict how changes in social behaviours and clinical care pathways during the pandemic might lead to increased liver disease incidence and severity.
Conflict of interest statement
A.S.B. has served as a consultant to Target RWE, Genfit and Intercept Pharmaceuticals. V.W.W. has served as a consultant or advisory board member for 3V-BIO, AbbVie, Allergan, Boehringer Ingelheim, Center for Outcomes Research in Liver Diseases, Echosens, Gilead Sciences, Hanmi Pharmaceutical, Intercept, Merck, Novartis, Novo Nordisk, Perspectum Diagnostics, Pfizer, ProSciento, Sagimet Biosciences, Taerget RWE, and Terns and as a speaker for AbbVie, Bristol-Myers Squibb, Echosens and Gilead Sciences. The remaining authors declare no competing interests.
Figures

References
-
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU) https://coronavirus.jhu.edu/map.html (2021).
-
- Berlin DA, Gulick RM, Martinez FJ. Severe Covid-19. N. Engl. J. Med. 2020;383:2451–2460. - PubMed
-
- World Health Organization. Clinical Management of COVID-19: Interim Guidance (2020).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
