

CT Angiography-Based Radiomics for Classification of Intracranial Aneurysm Rupture
- PMID: 33692741
- PMCID: PMC7937935
- DOI: 10.3389/fneur.2021.619864
CT Angiography-Based Radiomics for Classification of Intracranial Aneurysm Rupture
Abstract
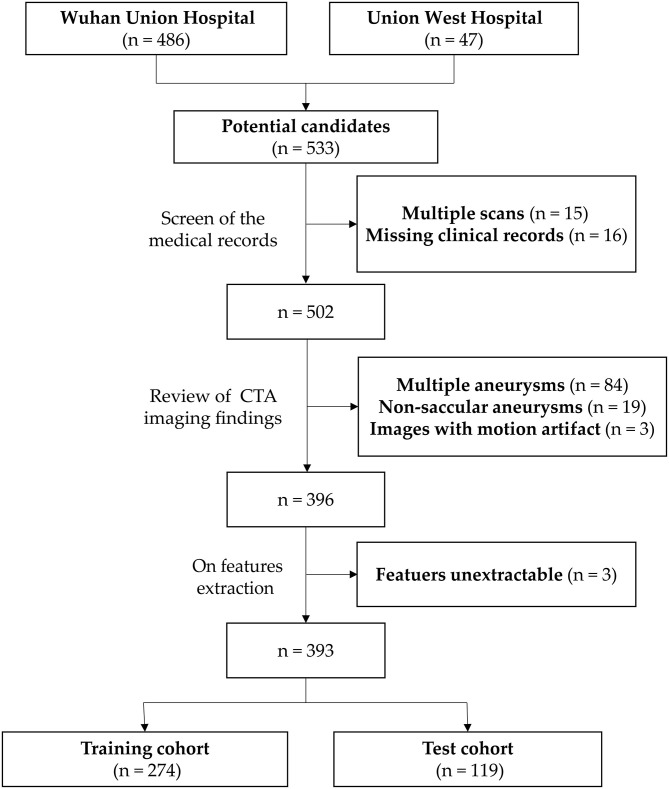
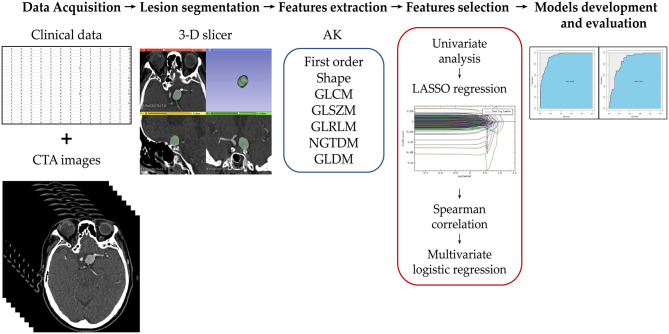
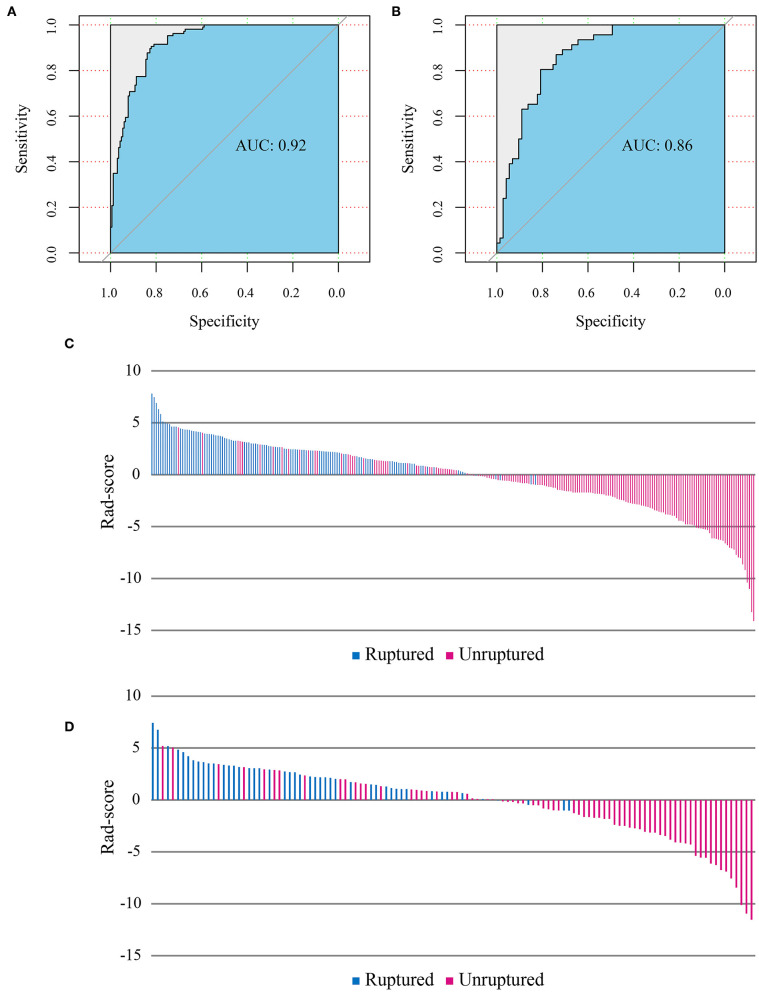
Background: Intracranial aneurysm rupture is a devastating medical event with a high morbidity and mortality rate. Thus, timely detection and management are critical. The present study aimed to identify the aneurysm radiomics features associated with rupture and to build and evaluate a radiomics classification model of aneurysm rupture. Methods: Radiomics analysis was applied to CT angiography (CTA) images of 393 patients [152 (38.7%) with ruptured aneurysms]. Patients were divided at a ratio of 7:3 into retrospective training (n = 274) and prospective test (n = 119) cohorts. A total of 1,229 radiomics features were automatically calculated from each aneurysm. The feature number was systematically reduced, and the most important classifying features were selected. A logistic regression model was constructed using the selected features and evaluated on training and test cohorts. Radiomics score (Rad-score) was calculated for each patient and compared between ruptured and unruptured aneurysms. Results: Nine radiomics features were selected from the CTA images and used to build the logistic regression model. The radiomics model has shown good performance in the classification of the aneurysm rupture on training and test cohorts [area under the receiver operating characteristic curve: 0.92 [95% confidence interval CI: 0.89-0.95] and 0.86 [95% CI: 0.80-0.93], respectively, p < 0.001]. Rad-score showed statistically significant differences between ruptured and unruptured aneurysms (median, 2.50 vs. -1.60 and 2.35 vs. -1.01 on training and test cohorts, respectively, p < 0.001). Conclusion: The results indicated the potential of aneurysm radiomics features for automatic classification of aneurysm rupture on CTA images.
Keywords: aneurysm rupture; intracranial aneurysm; machine learning; radiomics; subarachnoid hemorrhage.
Copyright © 2021 Alwalid, Long, Xie, Yang, Cen, Liu and Han.
Conflict of interest statement
HL was employed by GE Healthcare Company. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Thompson BG, Brown RD, Jr, Amin-Hanjani S, Broderick JP, Cockroft KM, Connolly ES, Jr, et al. Guidelines for the management of patients with unruptured intracranial aneurysms: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2015) 46:2368–400. 10.1161/STR.0000000000000070 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources