

Effects of Melatonin on Neurobehavior and Cognition in a Cerebral Palsy Model of plppr5-/- Mice
- PMID: 33692754
- PMCID: PMC7937640
- DOI: 10.3389/fendo.2021.598788
Effects of Melatonin on Neurobehavior and Cognition in a Cerebral Palsy Model of plppr5-/- Mice
Erratum in
-
Corrigendum: Effects of Melatonin on Neurobehavior and Cognition in a Cerebral Palsy Model of plppr5-/- Mice.Front Endocrinol (Lausanne). 2022 Mar 14;13:879685. doi: 10.3389/fendo.2022.879685. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35370970 Free PMC article.
Abstract
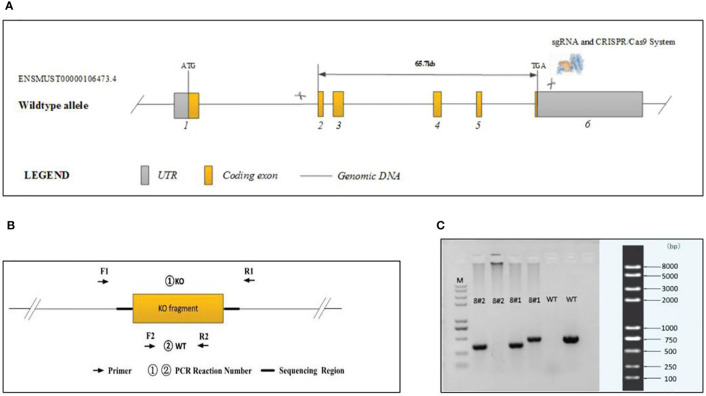
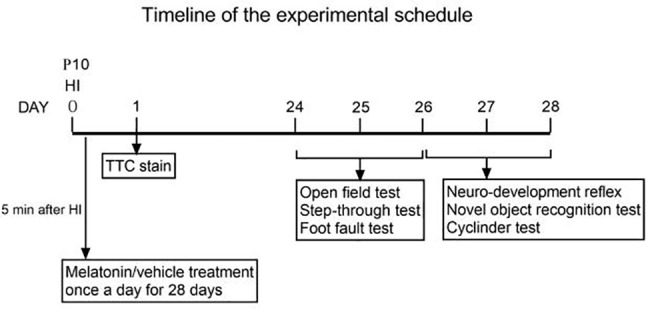
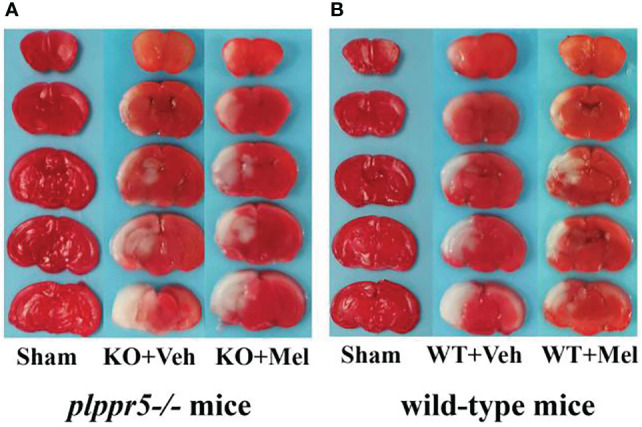
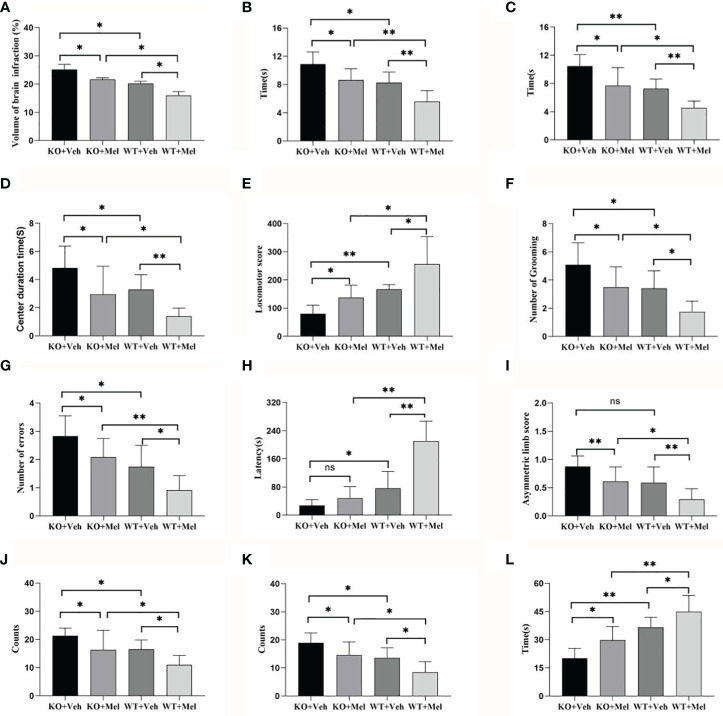
Cerebral palsy (CP), a group of clinical syndromes caused by non-progressive brain damage in the developing fetus or infant, is one of the most common causes of lifelong physical disability in children in most countries. At present, many researchers believe that perinatal cerebral hypoxic ischemic injury or inflammatory injury are the main causes of cerebral palsy. Previous studies including our works confirmed that melatonin has a protective effect against convulsive brain damage during development and that it affects the expression of various molecules involved in processes such as metabolism, plasticity and signaling in the brain. Integral membrane protein plppr5 is a new member of the plasticity-related protein family, which is specifically expressed in brain and spinal cord, and induces filopodia formation as well as neurite growth. It is highly expressed in the brain, especially in areas of high plasticity, such as the hippocampus. The signals are slightly lower in the cortex, the cerebellum, and in striatum. Noteworthy, during development plppr5 mRNA is expressed in the spinal cord, i.e., in neuron rich regions such as in medial motor nuclei, suggesting that plppr5 plays an important role in the regulation of neurons. However, the existing literature only states that plppr5 is involved in the occurrence and stability of dendritic spines, and research on its possible involvement in neonatal ischemic hypoxic encephalopathy has not been previously reported. We used plppr5 knockout (plppr5-/-) mice and their wild-type littermates to establish a model of hypoxicischemic brain injury (HI) to further explore the effects of melatonin on brain injury and the role of plppr5 in this treatment in an HI model, which mainly focuses on cognition, exercise, learning, and memory. All the tests were performed at 3-4 weeks after HI. As for melatonin treatment, which was performed 5 min after HI injury and followed by every 24h. In these experiments, we found that there was a significant interaction between genotype and treatment in novel object recognition tests, surface righting reflex tests and forelimb suspension reflex tests, which represent learning and memory, motor function and coordination, and the forelimb grip of the mice, respectively. However, a significant main effect of genotype and treatment on performance in all behavioral tests were observed. Specifically, wild-type mice with HI injury performed better than plppr5-/- mice, regardless of treatment with melatonin or vehicle. Moreover, treatment with melatonin could improve behavior in the tests for wild-type mice with HI injury, but not for plppr5-/- mice. This study showed that plppr5 knockout aggravated HI damage and partially weakened the neuroprotection of melatonin in some aspects (such as novel object recognition test and partial nerve reflexes), which deserves further study.
Keywords: cerebral palsy; hypoxic-ischemic; melatonin; neurobehavior; plppr5.
Copyright © 2021 Sun, Ma, Jin, Zheng, Wang and Ni.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Kirby RS, Wingate MS, Van Naarden Braun K, Doernberg NS, Arneson CL, Benedict RE, et al. Prevalence and functioning of children with cerebral palsy in four areas of the United States in 2006: a report from the Autism and Developmental Disabilities Monitoring Network. Res Dev Disabil (2011) 32:462–9. doi: 10.1016/j.ridd.2010.12.042 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous