

Prospects of Germline Nuclear Transfer in Women With Diminished Ovarian Reserve
- PMID: 33692760
- PMCID: PMC7937897
- DOI: 10.3389/fendo.2021.635370
Prospects of Germline Nuclear Transfer in Women With Diminished Ovarian Reserve
Abstract
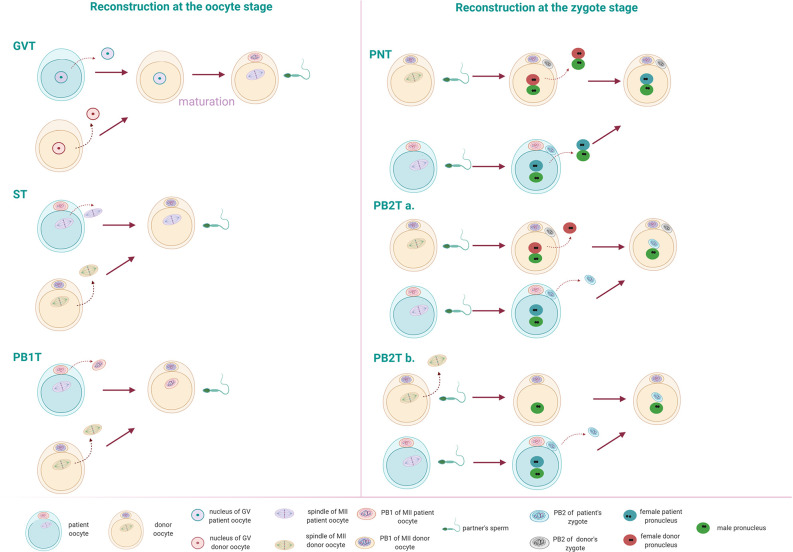
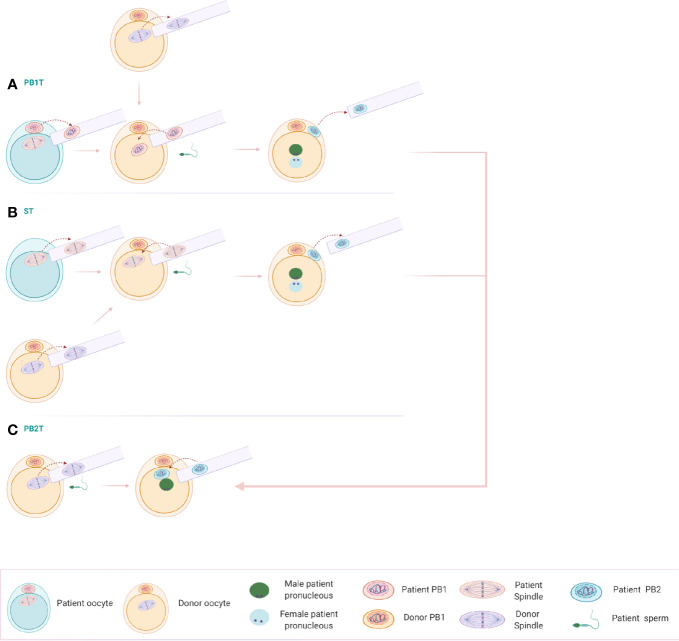
Diminished ovarian reserve (DOR) is associated with a reduced quantity and quality of the retrieved oocytes, usually leading to poor reproductive outcomes which remain a great challenge for assisted reproduction technology (ART). Women with DOR often have to seek for oocyte donation, precluding genetically related offspring. Germline nuclear transfer (NT) is a novel technology in ART that involves the transfer of the nuclear genome from an affected oocyte/zygote of the patient to the cytoplast of an enucleated donor oocyte/zygote. Therefore, it offers opportunities for the generation of genetically related embryos. Currently, although NT is clinically applied only in women with serious mitochondrial DNA disorders, this technology has also been proposed to overcome certain forms of female infertility, such as advanced maternal age and embryo developmental arrest. In this review, we are proposing the NT technology as a future treatment option for DOR patients. Strikingly, the application of different NT strategies will result in an increase of the total number of available reconstituted embryos for DOR patients.
Keywords: diminished ovarian reserve; germline nuclear transfer; oocyte quality; polar body transfer; poor ovarian response; spindle transfer.
Copyright © 2021 Christodoulaki, Boel, Tang, De Roo, Stoop and Heindryckx.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials