

Case Report: A Case of Acute Cellular Rejection Due to Atopic Dermatitis Exacerbation 3 Years After Heart Transplantation
- PMID: 33692803
- PMCID: PMC7937951
- DOI: 10.3389/fimmu.2021.630051
Case Report: A Case of Acute Cellular Rejection Due to Atopic Dermatitis Exacerbation 3 Years After Heart Transplantation
Abstract
Background: Little evidence has been presented about the association between previous atopic/allergic disease and graft rejection after solid organ transplantation. Thus, we present a case wherein acute cellular rejection (ACR) after heart transplantation (HTx) was noted along with exacerbation of atopic disease.
Case summary: A 32-year-old man was admitted at our hospital for regular monitoring of graft rejection. He had undergone heart transplant 3 years prior due to dilated cardiomyopathy. Echocardiogram revealed good biventricular function, and no abnormal findings were found in blood sampling tests. However, biopsy showed moderate ACR [Grade 2R(ISHLT 2004)/3A(ISHLT 1990)], which required twice-repeated steroid pulses with intensified immunosuppression. Meanwhile, his atopic dermatitis, which was diagnosed before having heart failure, was getting worse for the past 6 months. The exacerbation of atopic dermatitis was presumed to be related to the development of the intractable cellular rejection.
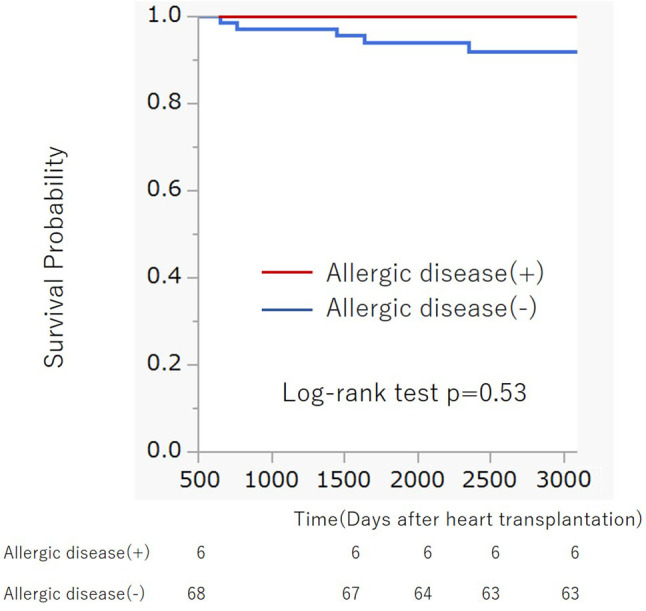
Discussion: This case suggested the association of atopic disease and graft rejection after HTx. We examined 76 patients from a cohort of previous studies who underwent HTx at our hospital, which suggested that patients with atopic/allergic disorders such as atopic dermatitis and asthma tended to have a significantly higher frequency of moderate rejection than non-allergic patients. (p = 0.012; Fisher's exact test). Our case also suggests that exacerbation of atopic dermatitis might cause graft rejection of the transplanted organ, so that it is important to carefully evaluate the risk of graft rejection if there is a previous history of atopic/allergic disease.
Keywords: acute cellular rejection; atopic dermatitis; heart transplantation; late rejection of graft; regulatory T cell.
Copyright © 2021 Kakuda, Amiya, Hatano, Maki, Bujo, Tsuji, Narita, Fujita, Ishida, Ono and Komuro.
Conflict of interest statement
EA and MH belong to the Department of Therapeutic Strategy for Heart Failure, Graduate School of Medicine, University of Tokyo, which is endowed by Actelion Pharmaceuticals Japan Ltd., Otsuka Pharmaceutical, NIPRO CORPORATION, Terumo Corp., Senko Medical Instrument Mfg., Century Medical Inc., Kinetic Concepts Inc., and St. Jude Medical. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous