

Comorbid neuropathological diagnoses in early versus late-onset Alzheimer's disease
- PMID: 33693619
- PMCID: PMC8502474
- DOI: 10.1093/brain/awab099
Comorbid neuropathological diagnoses in early versus late-onset Alzheimer's disease
Abstract
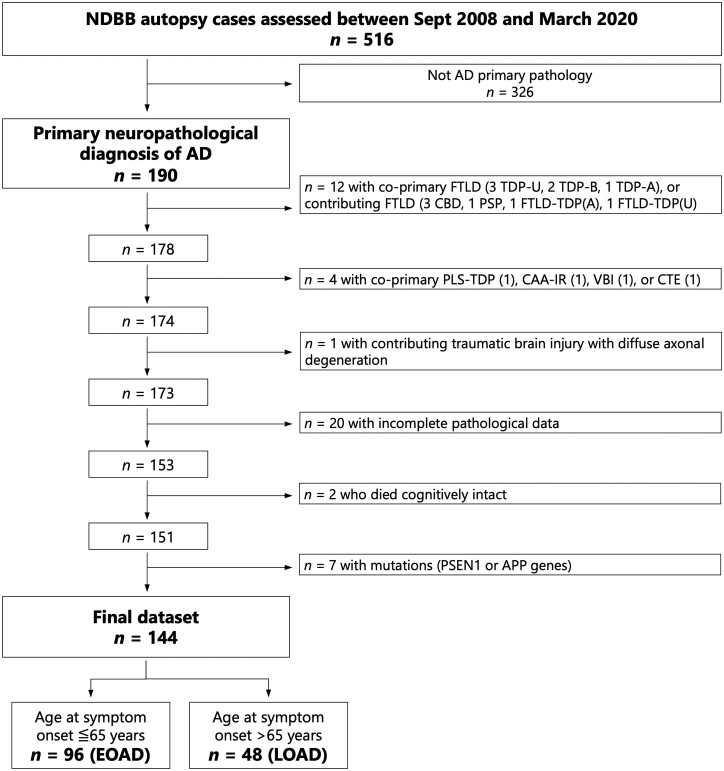
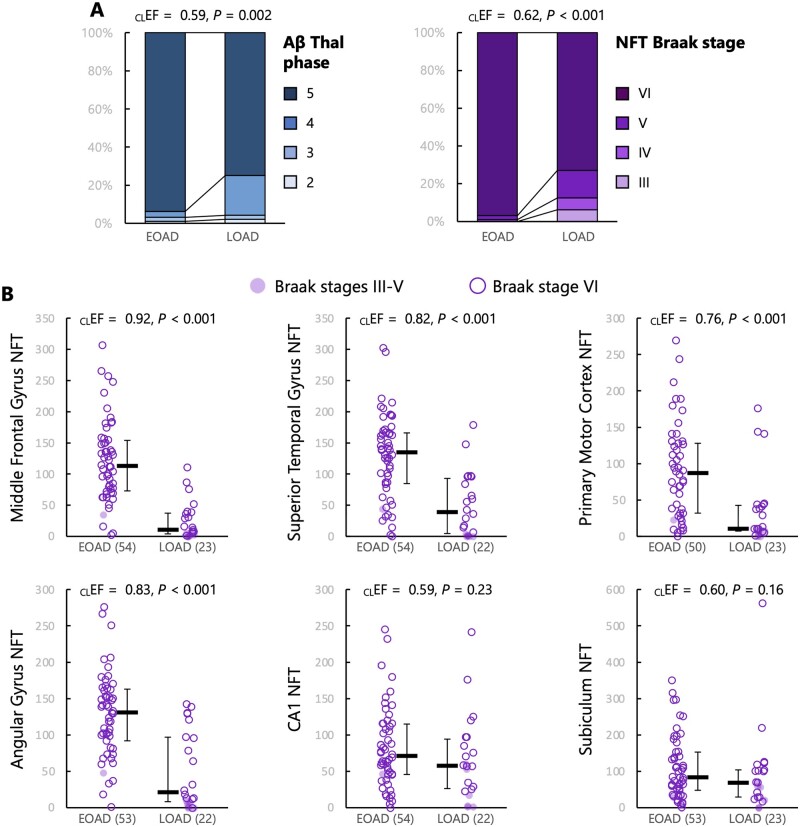
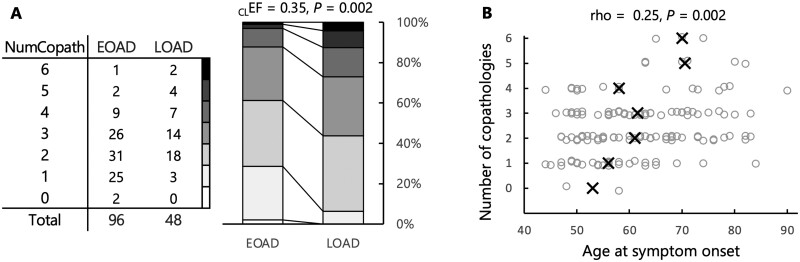
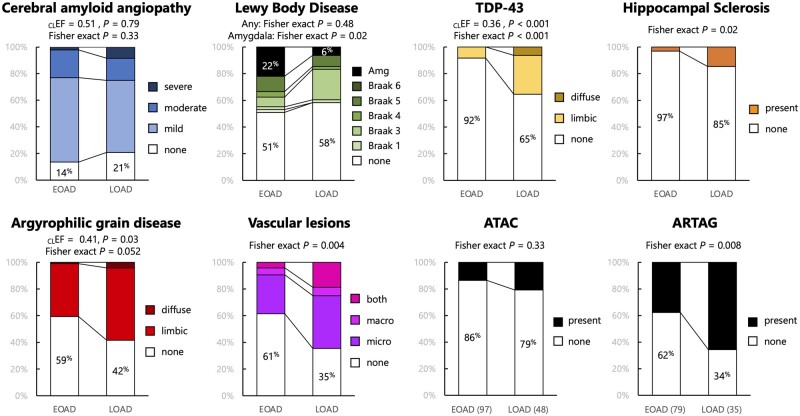
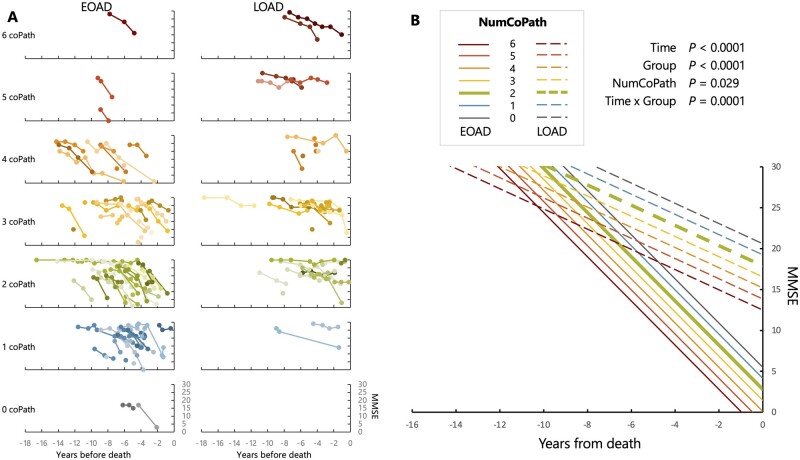
Co-pathologies play an important role in the expression of the Alzheimer's disease clinical phenotype and may influence treatment efficacy. Early-onset Alzheimer's disease, defined as manifesting before age 65, is viewed as a relatively pure form of Alzheimer's disease with a more homogeneous neuropathological substrate. We sought to compare the frequency of common neuropathological diagnoses in a consecutive autopsy series of 96 patients with early-onset Alzheimer's disease (median age of onset = 55 years, 44 females) and 48 with late-onset Alzheimer's disease (median age of onset = 73 years, 14 females). The UCSF Neurodegenerative Disease Brain Bank database was reviewed to identify patients with a primary pathological diagnosis of Alzheimer's disease. Prevalence and stage of Lewy body disease, limbic age-related TDP-43 encephalopathy (LATE), argyrophilic grain disease, hippocampal sclerosis, cerebral amyloid angiopathy, and vascular brain injury were compared between the two cohorts. We found at least one non-Alzheimer's disease pathological diagnosis in 98% of patients with early-onset Alzheimer's disease (versus 100% of late onset), and the number of comorbid diagnoses per patient was lower in early-onset than in late-onset Alzheimer's disease (median = 2 versus 3, Mann-Whitney Z = 3.00, P = 0.002). Lewy body disease and cerebral amyloid angiopathy were common in both early and late onset Alzheimer's disease (cerebral amyloid angiopathy: 86% versus 79%, Fisher exact P = 0.33; Lewy body disease: 49% versus 42%, P = 0.48, respectively), although amygdala-predominant Lewy body disease was more common in early than late onset Alzheimer's disease (22% versus 6%, P = 0.02). In contrast, LATE (35% versus 8%, P < 0.001), hippocampal sclerosis (15% versus 3%, P = 0.02), argyrophilic grain disease (58% versus 41%, P = 0.052), and vascular brain injury (65% versus 39%, P = 0.004) were more common in late than in early onset Alzheimer's disease, respectively. The number of co-pathologies predicted worse cognitive performance at the time of death on Mini-Mental State Examination [1.4 points/pathology (95% confidence interval, CI -2.5 to -0.2) and Clinical Dementia Rating-Sum of Boxes (1.15 point/pathology, 95% CI 0.45 to 1.84)], across early and late onset cohorts. The effect of sex on the number of co-pathologies was not significant (P = 0.17). Prevalence of at least one APOE ε4 allele was similar across the two cohorts (52% and 54%) and was associated with a greater number of co-pathologies (+0.40, 95% CI 0.01 to 0.79, P = 0.047), independent of age of symptom onset, sex, and disease duration. Females showed higher density of neurofibrillary tangles compared to males, controlling for age of onset, APOE ε4, and disease duration. Our findings suggest that non-Alzheimer's disease pathological diagnoses play an important role in the clinical phenotype of early onset Alzheimer's disease with potentially significant implications for clinical practice and clinical trials design.
Keywords: Alzheimer's disease; Apo E; copathologies; early-onset; late-onset.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Coulthard EJ, Love S.. A broader view of dementia: Multiple co-pathologies are the norm. Brain. 2018;141(7):1894–1897. - PubMed
-
- Higashi S, Iseki E, Yamamoto R, et al. Concurrence of TDP-43, tau and alpha-synuclein pathology in brains of Alzheimer’s disease and dementia with Lewy bodies. Brain Res. 2007;1184:284–294. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 AG057195/AG/NIA NIH HHS/United States
- K24 AG053435/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- K99 AG065501/AG/NIA NIH HHS/United States
- K08 AG052648/AG/NIA NIH HHS/United States
- P01-AG019724/Alzheimer's Disease Research Center
- K08 NS114170/NS/NINDS NIH HHS/United States
- R01 AG045611/AG/NIA NIH HHS/United States
- P30-AG062422/National Institute for Health
- U54 NS100717/NS/NINDS NIH HHS/United States
- K24 AG045333/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
