

Reduced Trypanosoma cruzi-specific humoral response and enhanced T cell immunity after treatment interruption with benznidazole in chronic Chagas disease
- PMID: 33693664
- PMCID: PMC8600036
- DOI: 10.1093/jac/dkab054
Reduced Trypanosoma cruzi-specific humoral response and enhanced T cell immunity after treatment interruption with benznidazole in chronic Chagas disease
Abstract
Background: Interruption of benznidazole therapy due to the appearance of adverse effects, which is presumed to lead to treatment failure, is a major drawback in the treatment of chronic Chagas disease.
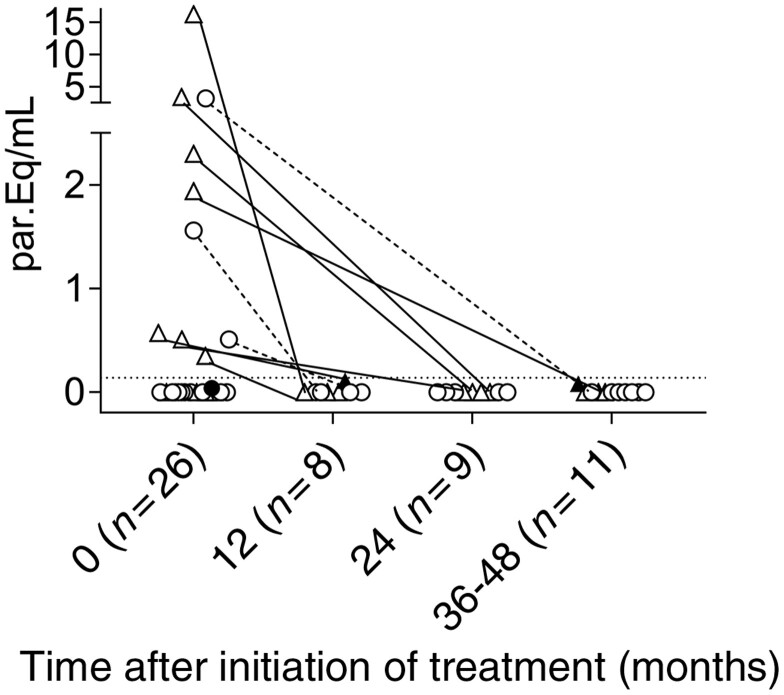
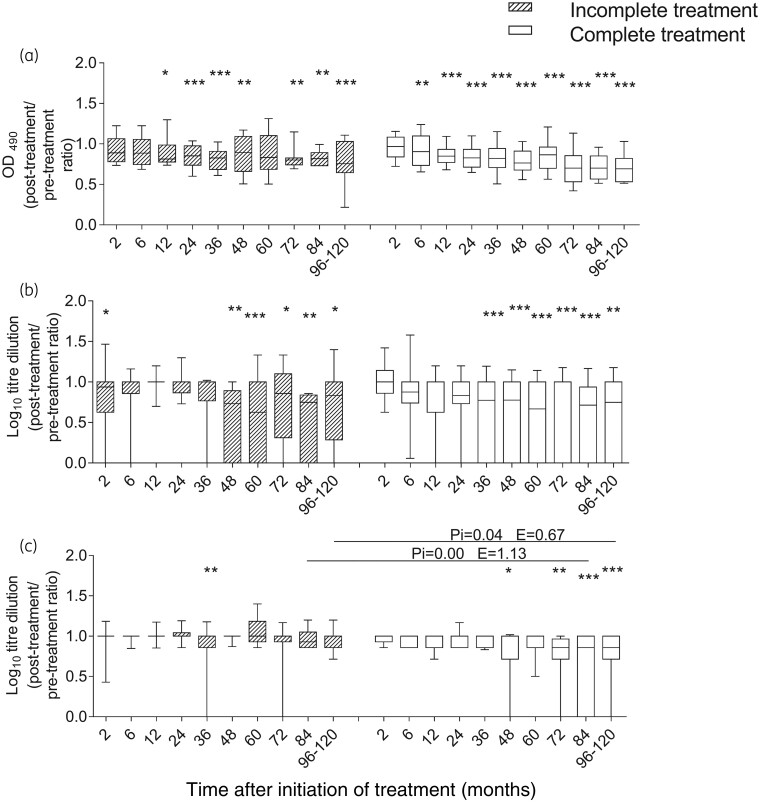
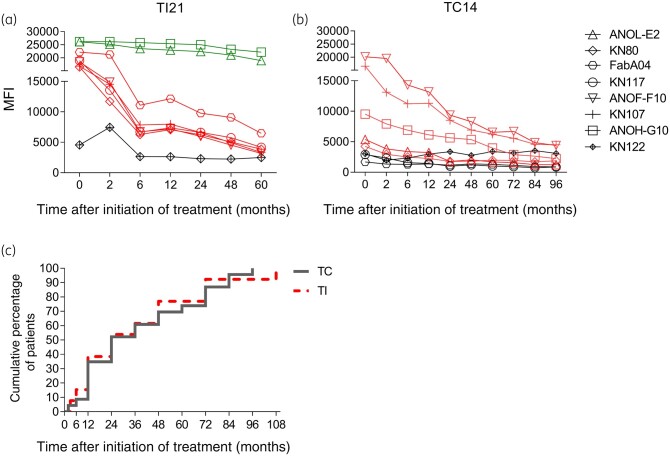
Methods: Trypanosoma cruzi-specific humoral and T cell responses, T cell phenotype and parasite load were measured to compare the outcome in 33 subjects with chronic Chagas disease treated with an incomplete benznidazole regimen and 58 subjects treated with the complete regimen, during a median follow-up period of 48 months.
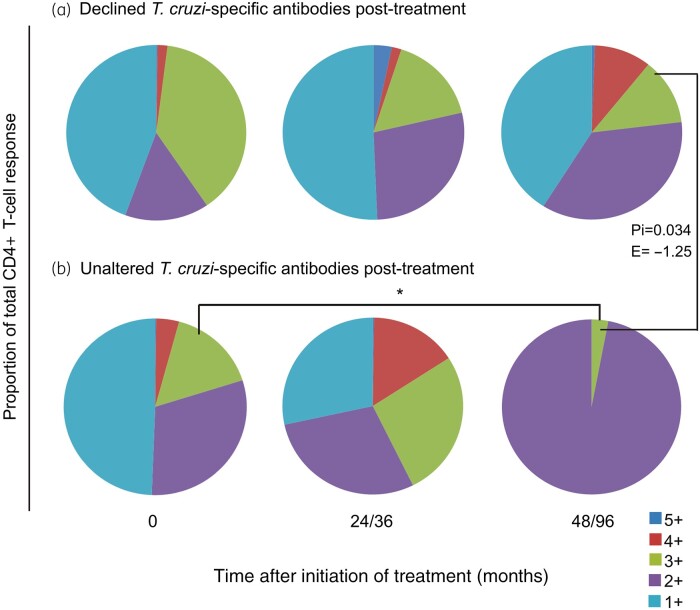
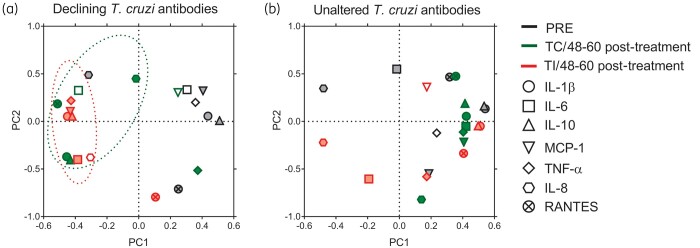
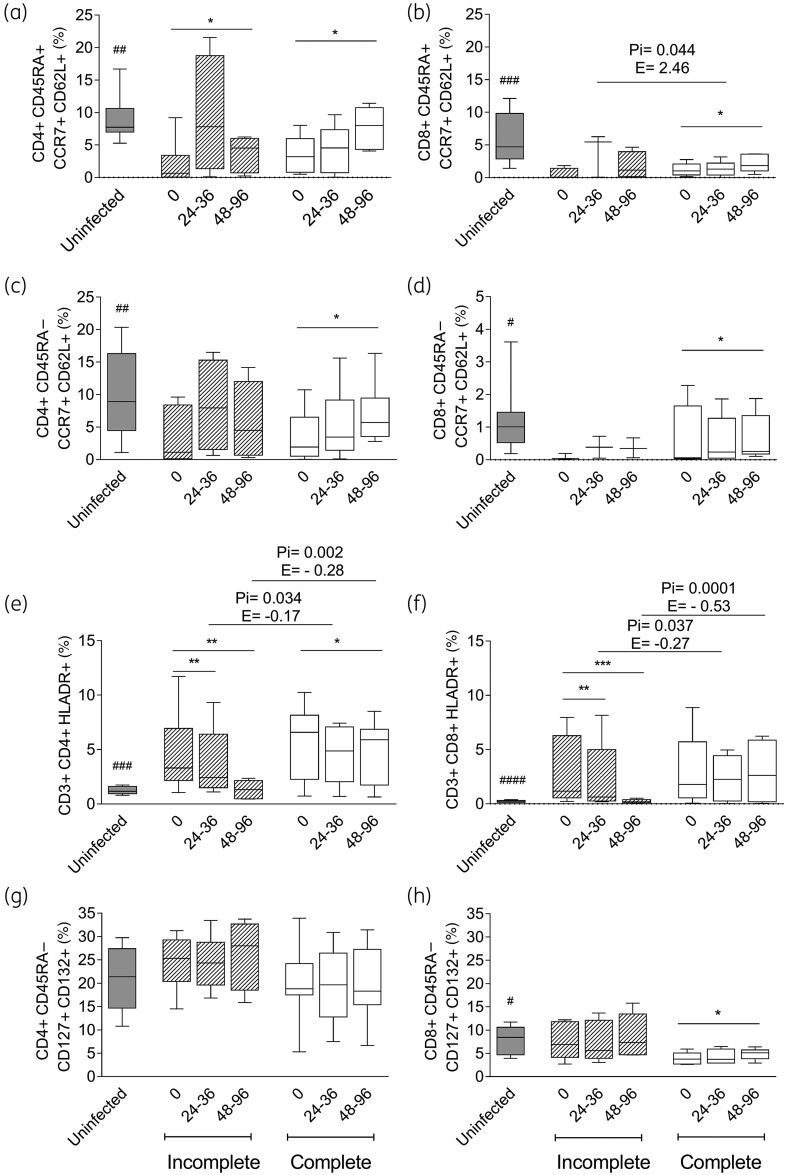
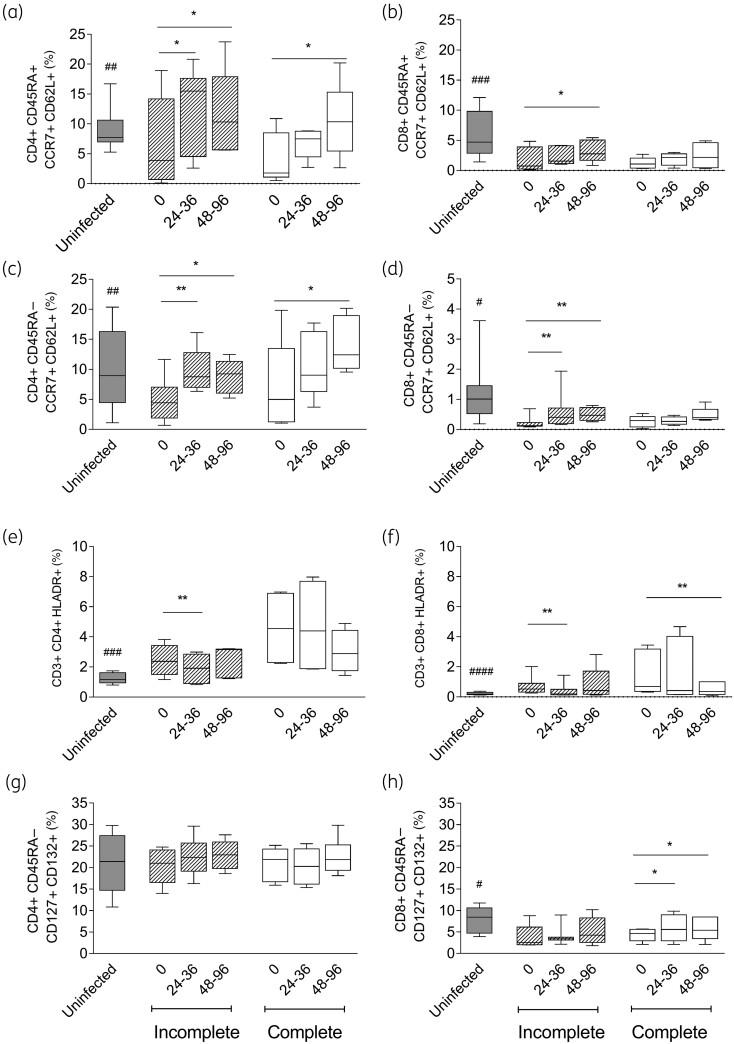
Results: Both treatment regimens induced a reduction in the T. cruzi-specific antibody levels and similar rates of treatment failure when evaluated using quantitative PCR. Regardless of the regimen, polyfunctional CD4+ T cells increased in the subjects, with successful treatment outcome defined as a decrease of T. cruzi-specific antibodies. Regardless of the serological outcome, naive and central memory T cells increased after both regimens. A decrease in CD4+ HLA-DR+ T cells was associated with successful treatment in both regimens. The cytokine profiles of subjects with successful treatment showed fewer inflammatory mediators than those of the untreated T. cruzi-infected subjects. High levels of T cells expressing IL-7 receptor and low levels of CD8+ T cells expressing the programmed cell death protein 1 at baseline were associated with successful treatment following benznidazole interruption.
Conclusions: These findings challenge the notion that treatment failure is the sole potential outcome of an incomplete benznidazole regimen and support the need for further assessment of the treatment protocols for chronic Chagas disease.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- WHO. Chagas disease (also known as American trypanosomiasis). 2018. http://www.who.int/news-room/fact-sheets/detail/chagas-disease-(american...).
-
- Antinori S, Galimberti L, Bianco R. et al. Chagas disease in Europe: a review for the internist in the globalized world. Eur J Intern Med 2017; 43: 6–15. - PubMed
-
- Ministerio de Salud Argentina. Guías para la atención al paciente infectado con Trypanosoma cruzi (Enfermedad de Chagas). https://bancos.salud.gob.ar/recurso/guias-para-la-atencion-al-paciente-i....
-
- Viotti R, Vigliano C, Lococo B. et al. Side effects of benznidazole as treatment in chronic Chagas disease: fears and realities. Expert Rev Anti Infect Ther 2009; 7: 157–63. - PubMed
-
- Crespillo-Andújar C, Venanzi-Rullo E, López-Vélez R. et al. Safety profile of benznidazole in the treatment of chronic Chagas disease: experience of a referral centre and systematic literature review with meta-analysis. Drug Saf 2018; 41: 1035–48. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
