

Attributable mortality of ICU acquired bloodstream infections: a propensity-score matched analysis
- PMID: 33694037
- PMCID: PMC7945601
- DOI: 10.1007/s10096-021-04215-4
Attributable mortality of ICU acquired bloodstream infections: a propensity-score matched analysis
Abstract
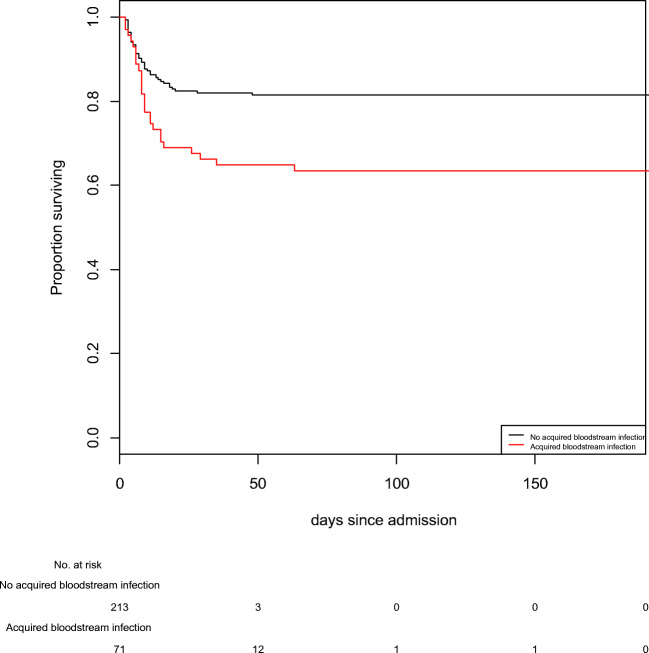
The mortality attributable to ICU-acquired bloodstream infection (BSI) differs between studies due to statistical methods used for cohort matching. Propensity-score matching has never been used to avoid eventual bias when studying BSI attributable mortality in the ICU. We conducted an observational prospective study over a 4-year period, on patients admitted for at least 48 h in 2 intensive care units. Based on risk factors for death in the ICU and for BSI, each patient with BSI was matched with 3 patients without BSI using propensity-score matching. We performed a competitive risk analysis to study BSI mortality attributable fraction. Of 2464 included patients, 71 (2.9%) had a BSI. Propensity-score matching was highly effective and group characteristics were fully balanced. Crude mortality was 36.6% in patients with BSI and 21.6% in propensity-score matched patients (p=0.018). Attributable mortality of BSI was 2.3% [1.2-4.0] and number needed to harm was 6.7. With Fine and Gray model, a higher risk for death was observed in patients with BSI than in propensity-score matched patients (sub distribution Hazard Ratio (sdHR) = 2.11; 95% CI [1.32-3.37] p = 0.002). Patients with BSI had a higher risk for death and BSI attributable mortality fraction was 2.3%.
Keywords: Bacteremia; Critical care; Mortality; Propensity score.
© 2021. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The authors declare that they have no conflict of interest.
References
-
- Adrie C, Garrouste-Orgeas M, Ibn Essaied W, Schwebel C, Darmon M, Mourvillier B, et al. Attributable mortality of ICU-acquired bloodstream infections: impact of the source, causative micro-organism, resistance profile and antimicrobial therapy. J Inf Secur. 2017;74:131–141. - PubMed
-
- Higuera F, Rangel-Frausto MS, Rosenthal VD, Soto JM, Castañon J, Franco G, Tabal-Galan N, Ruiz J, Duarte P, Graves N. Attributable cost and length of stay for patients with central venous catheter-associated bloodstream infection in Mexico City intensive care units: a prospective, matched analysis. Infect Control Hosp Epidemiol. 2007;28:31–35. doi: 10.1086/510812. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
