

Benefit, Harm, and Cost-effectiveness Associated With Magnetic Resonance Imaging Before Biopsy in Age-based and Risk-stratified Screening for Prostate Cancer
- PMID: 33704474
- PMCID: PMC7953309
- DOI: 10.1001/jamanetworkopen.2020.37657
Benefit, Harm, and Cost-effectiveness Associated With Magnetic Resonance Imaging Before Biopsy in Age-based and Risk-stratified Screening for Prostate Cancer
Abstract
Importance: If magnetic resonance imaging (MRI) mitigates overdiagnosis of prostate cancer while improving the detection of clinically significant cases, including MRI in a screening program for prostate cancer could be considered.
Objective: To evaluate the benefit-harm profiles and cost-effectiveness associated with MRI before biopsy compared with biopsy-first screening for prostate cancer using age-based and risk-stratified screening strategies.
Design, setting, and participants: This decision analytical model used a life-table approach and was conducted between December 2019 and July 2020. A hypothetical cohort of 4.48 million men in England aged 55 to 69 years were analyzed and followed-up to 90 years of age.
Exposures: No screening, age-based screening, and risk-stratified screening in the hypothetical cohort. Age-based screening consisted of screening every 4 years with prostate-specific antigen between the ages of 55 and 69 years. Risk-stratified screening used age and polygenic risk profiles.
Main outcomes and measures: The benefit-harm profile (deaths from prostate cancer, quality-adjusted life-years, overdiagnosis, and biopsies) and cost-effectiveness (net monetary benefit, from a health care system perspective) were analyzed. Both age-based and risk-stratified screening were evaluated using a biopsy-first and an MRI-first diagnostic pathway. Results were derived from probabilistic analyses and were discounted at 3.5% per annum.
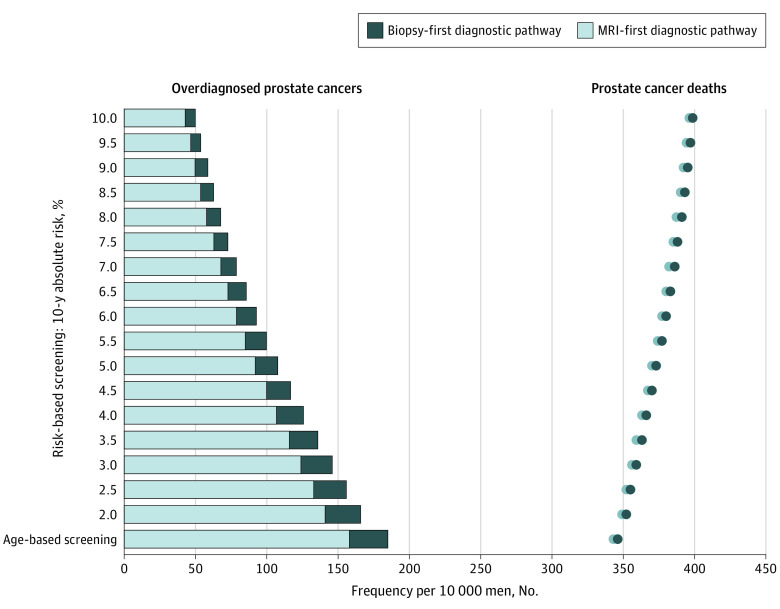
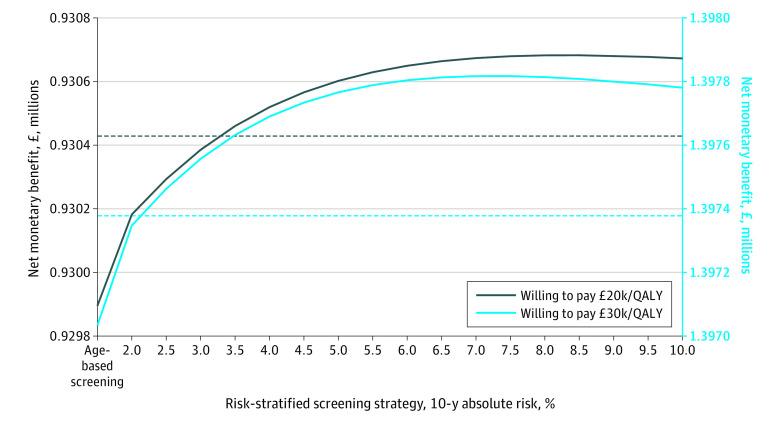
Results: The hypothetical cohort included 4.48 million men in England, ranging in age from 55 to 69 years (median, 62 years). Compared with biopsy-first age-based screening, MRI-first age-based screening was associated with 0.9% (1368; 95% uncertainty interval [UI], 1370-1409) fewer deaths from prostate cancer, 14.9% (12 370; 95% UI, 11 100-13 670) fewer overdiagnoses, and 33.8% (650 500; 95% UI, 463 200-907 000) fewer biopsies. At 10-year absolute risk thresholds of 2% and 10%, MRI-first risk-stratified screening was associated with between 10.4% (7335; 95% UI, 6630-8098) and 72.6% (51 250; 95% UI, 46 070-56 890) fewer overdiagnosed cancers, respectively, and between 21.7% fewer MRIs (412 100; 95% UI, 411 400-412 900) and 53.5% fewer biopsies (1 016 000; 95% UI, 1 010 000-1 022 000), respectively, compared with MRI-first age-based screening. The most cost-effective strategies at willingness-to-pay thresholds of £20 000 (US $26 000) and £30 000 (US $39 000) per quality-adjusted life-year gained were MRI-first risk-stratified screening at 10-year absolute risk thresholds of 8.5% and 7.5%, respectively.
Conclusions and relevance: In this decision analytical model of a hypothetical cohort, an MRI-first diagnostic pathway was associated with an improvement in the benefit-harm profile and cost-effectiveness of screening for prostate cancer compared with biopsy-first screening. These improvements were greater when using risk-stratified screening based on age and polygenic risk profile and may warrant prospective evaluation.
Conflict of interest statement
Figures
Comment in
-
Prostate Cancer Screening-The Need for and Clinical Relevance of Decision Analytical Models.JAMA Netw Open. 2021 Mar 1;4(3):e212182. doi: 10.1001/jamanetworkopen.2021.2182. JAMA Netw Open. 2021. PMID: 33704471 No abstract available.
References
-
- Faria R, Soares MO, Spackman E, et al. . Optimising the diagnosis of prostate cancer in the era of multiparametric magnetic resonance imaging: a cost-effectiveness analysis based on the Prostate MR Imaging Study (PROMIS). Eur Urol. 2018;73(1):23-30. doi:10.1016/j.eururo.2017.08.018 - DOI - PMC - PubMed
-
- Elwenspoek MMC, Sheppard AL, McInnes MDF, et al. . Comparison of multiparametric magnetic resonance imaging and targeted biopsy with systematic biopsy alone for the diagnosis of prostate cancer: a systematic review and meta-analysis. JAMA Netw Open. 2019;2(8):e198427. doi:10.1001/jamanetworkopen.2019.8427 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
