

The hidden curve behind COVID-19 outbreak: the impact of delay in treatment initiation in cancer patients and how to mitigate the additional risk of dying-the head and neck cancer model
- PMID: 33704627
- PMCID: PMC7950430
- DOI: 10.1007/s10552-021-01411-7
The hidden curve behind COVID-19 outbreak: the impact of delay in treatment initiation in cancer patients and how to mitigate the additional risk of dying-the head and neck cancer model
Abstract
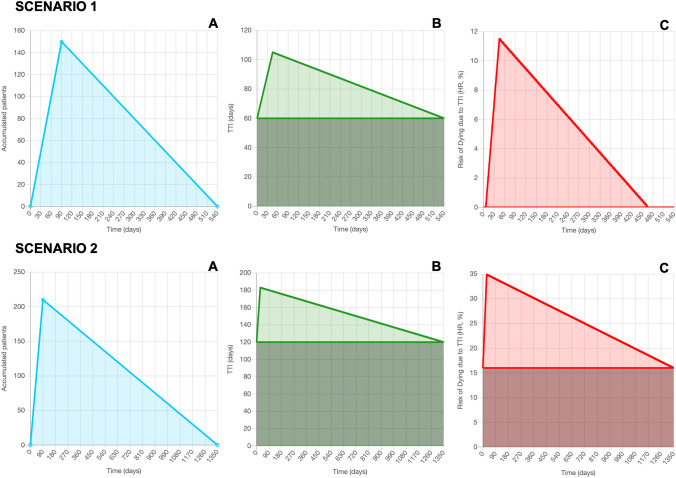
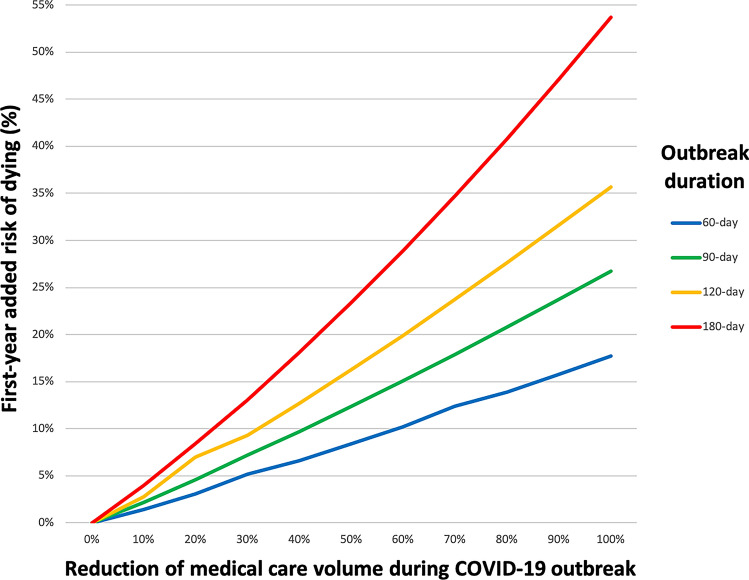
Purpose: The rapid spread of the SARS-CoV-2 pandemic around the world caused most healthcare services to turn substantial attention to treatment of these patients and also to alter the structure of healthcare systems to address an infectious disease. As a result, many cancer patients had their treatment deferred during the pandemic, increasing the time-to-treatment initiation, the number of untreated patients (which will alter the dynamics of healthcare delivery in the post-pandemic era) and increasing their risk of death. Hence, we analyzed the impact on global cancer mortality considering the decline in oncology care during the COVID-19 outbreak using head and neck cancer, a known time-dependent disease, as a model.
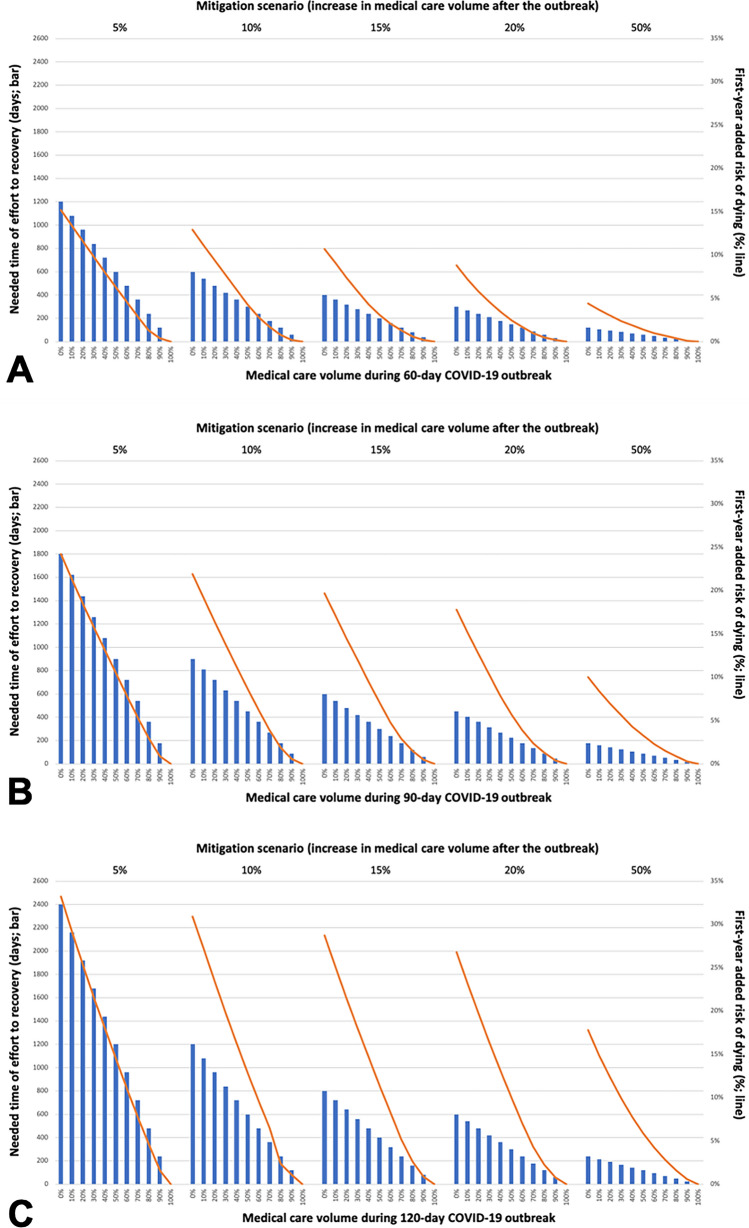
Methods: An online practical tool capable of predicting the risk of cancer patients dying due to the COVID-19 outbreak and also useful for mitigation strategies after the peak of the pandemic has been developed, based on a mathematical model. The scenarios were estimated by information of 15 oncological services worldwide, given a perspective from the five continents and also some simulations were conducted at world demographic data.
Results: The model demonstrates that the more that cancer care was maintained during the outbreak and also the more it is increased during the mitigation period, the shorter will be the recovery, lessening the additional risk of dying due to time-to-treatment initiation.
Conclusions: This impact of COVID-19 pandemic on cancer patients is inevitable, but it is possible to minimize it with an effort measured by the proposed model.
Keywords: COVID-19; Head and Neck Neoplasms; Mortality; Risk Evaluation and Mitigation; Time-to-Treatment.
Conflict of interest statement
Hisham Mehanna is the director and a shareholder of Warwickshire Head and Neck Clinic LTD, he also reports personal fees from AstraZeneca, personal fees from MSD, personal fees from Sanofi Pasteur, personal fees from Merck, grants from GSK Biologicals, grants from MSD, grants from Sanofi Pasteur, grants from AstraZeneca, non-financial support from Merck, non-financial support from MSD, all disclosures are outside the submitted work. Leandro L. Matos, Carlos Henrique Q. Forster, Gustavo N. Marta, Gilberto Castro Junior, John A. Ridge, Daisy Hirata, Adalberto Miranda-Filho, Ali Hosny, Alvaro Sanabria, Vincent Gregoire, Snehal G. Patel, Johannes J. Fagan, Anil K. D’Cruz, Lisa Licitra, Sheng-Po Hao, Amanda Psyrri, Sandro Porceddu, Thomas J. Galloway, Wojciech Golusinski, Nancy Y. Lee, Elcio H. Shiguemori, José Elias Matieli, Ana Paula A. C. Shiguemori, Letícia R. Diamantino, Luiz Felipe Schiaveto, Lysia Leão, Ana F. Castro, André Lopes Carvalho, Luiz Paulo Kowalski declare that they have no conflict of interest.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
