

Awake Proning as an Adjunctive Therapy for Refractory Hypoxemia in Non-Intubated Patients with COVID-19 Acute Respiratory Failure: Guidance from an International Group of Healthcare Workers
- PMID: 33705348
- PMCID: PMC8103477
- DOI: 10.4269/ajtmh.20-1445
Awake Proning as an Adjunctive Therapy for Refractory Hypoxemia in Non-Intubated Patients with COVID-19 Acute Respiratory Failure: Guidance from an International Group of Healthcare Workers
Abstract
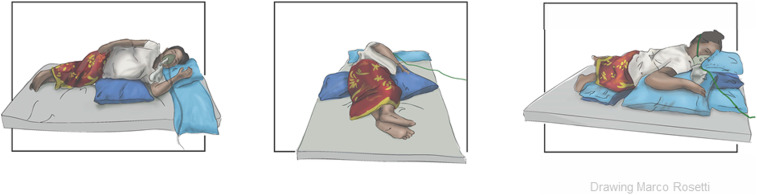
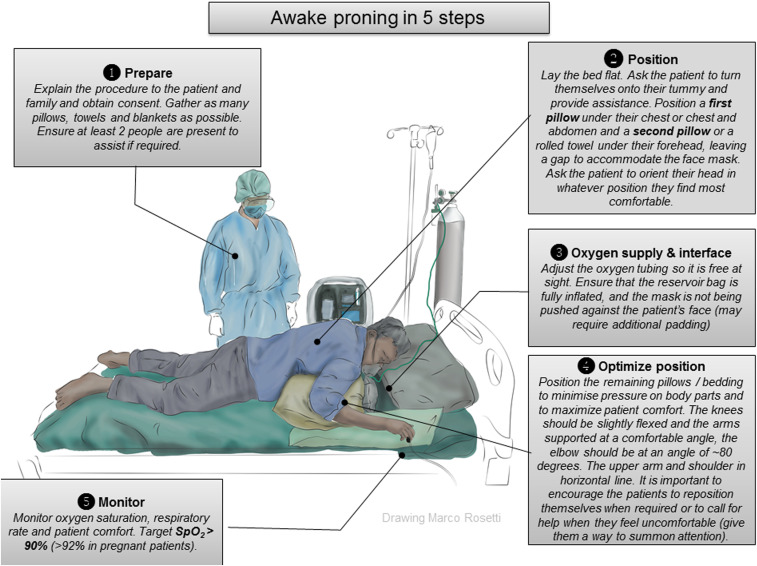
Non-intubated patients with acute respiratory failure due to COVID-19 could benefit from awake proning. Awake proning is an attractive intervention in settings with limited resources, as it comes with no additional costs. However, awake proning remains poorly used probably because of unfamiliarity and uncertainties regarding potential benefits and practical application. To summarize evidence for benefit and to develop a set of pragmatic recommendations for awake proning in patients with COVID-19 pneumonia, focusing on settings where resources are limited, international healthcare professionals from high and low- and middle-income countries (LMICs) with known expertise in awake proning were invited to contribute expert advice. A growing number of observational studies describe the effects of awake proning in patients with COVID-19 pneumonia in whom hypoxemia is refractory to simple measures of supplementary oxygen. Awake proning improves oxygenation in most patients, usually within minutes, and reduces dyspnea and work of breathing. The effects are maintained for up to 1 hour after turning back to supine, and mostly disappear after 6-12 hours. In available studies, awake proning was not associated with a reduction in the rate of intubation for invasive ventilation. Awake proning comes with little complications if properly implemented and monitored. Pragmatic recommendations including indications and contraindications were formulated and adjusted for resource-limited settings. Awake proning, an adjunctive treatment for hypoxemia refractory to supplemental oxygen, seems safe in non-intubated patients with COVID-19 acute respiratory failure. We provide pragmatic recommendations including indications and contraindications for the use of awake proning in LMICs.
Figures
References
-
- Wiersinga WJ, Prescott HC, 2020. What is COVID-19? JAMA 324: 816. - PubMed
-
- Ayzac L, Girard R, Baboi L, Beuret P, Rabilloud M, Richard JC, Guérin C, 2016. Ventilator-associated pneumonia in ARDS patients: the impact of prone positioning. A secondary analysis of the PROSEVA trial. Intensive Care Med 42: 871–878. - PubMed
-
- Scaravilli V, Grasselli G, Castagna L, Zanella A, Isgrò S, Lucchini A, Patroniti N, Bellani G, Pesenti A, 2015. Prone positioning improves oxygenation in spontaneously breathing nonintubated patients with hypoxemic acute respiratory failure: a retrospective study. J Crit Care 30: 1390–1394. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
