

Association between continuity of care and subsequent diagnosis of multimorbidity in Ontario, Canada from 2001-2015: A retrospective cohort study
- PMID: 33705429
- PMCID: PMC7951913
- DOI: 10.1371/journal.pone.0245193
Association between continuity of care and subsequent diagnosis of multimorbidity in Ontario, Canada from 2001-2015: A retrospective cohort study
Abstract
Background: Continuity of care is a well-recognized principle of the primary care discipline owing to its medical, interpersonal, and cost-saving benefits. Relationship continuity or the ongoing therapeutic relationship between a patient and their physician is a particularly desirable goal, but its role in preventing the accumulation of chronic conditions diagnoses in individuals is unknown. The objective of this study was to investigate the effect of continuity of care with physicians on the rate of incident multimorbidity diagnoses in patients with existing conditions.
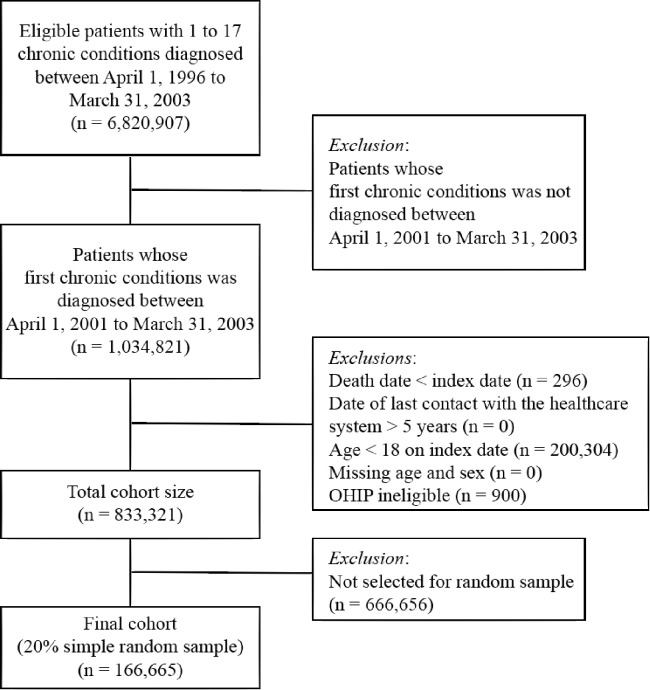
Methods: This was a population-based, retrospective cohort study from 2001 to 2015 that focused on patients aged 18 to 105 years with at least one chronic condition (n = 166,665). Our primary exposure was relationship continuity of care with general practitioners and specialists measured using the Bice-Boxerman Continuity of Care Index (COCI). COCI was specified as a time-dependent exposure prior to the observation period. Our outcomes of interest were the time to diagnosis of a second, third, and fourth chronic condition estimated using cause-specific hazard regressions accounting for death as a competing risk.
Findings: We observed that patients with a single chronic condition and high continuity of care (>0.50) were diagnosed with a second chronic condition or multimorbidity at an 8% lower rate compared to individuals with low continuity (cause-specific hazard ratio (HR) 0.92 (95% Confidence Interval 0.90-0.93; p<0.0001) after adjusting for age, sex, income, place of residence, primary care enrolment, and the annual number of physician visits. Continuity remained protective as the degree of multimorbidity increased. Among patients with two conditions, the risk of diagnosis of a third chronic condition was also 8% lower for individuals with high continuity (HR 0.92; CI 0.90-0.94; p<0.0001). Patients with three conditions and high continuity had a 9% lower risk of diagnosis with a fourth condition (HR 0.91; CI 0.89-0.93; p<0.0001).
Conclusions: Continuity of care is a potentially modifiable health system factor that reduces the rate at which diagnoses of chronic conditions are made over time in patients with multimorbidity. Additional research is needed to explain the underlying mechanisms through which continuity is related to a protective effect and the clinical sequalae.
Conflict of interest statement
All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: LCR is supported by a Canada Research Chair in Population Health Analytics. LCR and WPW are supported by Research Chairs funded by the Trillium Health Partners Foundation.
Figures
Similar articles
-
The association between multimorbidity and hospitalization is modified by individual demographics and physician continuity of care: a retrospective cohort study.BMC Health Serv Res. 2016 Apr 27;16:154. doi: 10.1186/s12913-016-1415-5. BMC Health Serv Res. 2016. PMID: 27122051 Free PMC article.
-
Effects of continuity of care on the postradiotherapy survival of working-age patients with oral cavity cancer: A nationwide population-based cohort study in Taiwan.PLoS One. 2019 Dec 16;14(12):e0225635. doi: 10.1371/journal.pone.0225635. eCollection 2019. PLoS One. 2019. PMID: 31841525 Free PMC article.
-
Multimorbidity and healthcare utilization among home care clients with dementia in Ontario, Canada: A retrospective analysis of a population-based cohort.PLoS Med. 2017 Mar 7;14(3):e1002249. doi: 10.1371/journal.pmed.1002249. eCollection 2017 Mar. PLoS Med. 2017. PMID: 28267802 Free PMC article.
-
Association of Primary Care Involvement with Death or Hospitalizations for Patients Starting Dialysis.Clin J Am Soc Nephrol. 2020 Apr 7;15(4):521-529. doi: 10.2215/CJN.10890919. Epub 2020 Mar 5. Clin J Am Soc Nephrol. 2020. PMID: 32139363 Free PMC article.
-
Primary medical care continuity and patient mortality: a systematic review.Br J Gen Pract. 2020 Aug 27;70(698):e600-e611. doi: 10.3399/bjgp20X712289. Print 2020 Sep. Br J Gen Pract. 2020. PMID: 32784220 Free PMC article.
Cited by
-
Typologie des soins primaires virtuels au Canada: Clarifier les répercussions.Can Fam Physician. 2024 Nov-Dec;70(11-12):e180-e186. doi: 10.46747/cfp.701112e180. Can Fam Physician. 2024. PMID: 39638392 Free PMC article. French. No abstract available.
-
Relational Continuity of Chronic Patients with Primary and Secondary Care Doctors: A Study of Public Healthcare Networks of Six Latin American Countries.Int J Environ Res Public Health. 2022 Oct 11;19(20):13008. doi: 10.3390/ijerph192013008. Int J Environ Res Public Health. 2022. PMID: 36293587 Free PMC article.
-
Transformation to a patient-centred medical home led and delivered by an urban Aboriginal and Torres Strait Islander community, and association with engagement and quality-of-care: quantitative findings from a pilot study.BMC Health Serv Res. 2023 Sep 6;23(1):959. doi: 10.1186/s12913-023-09955-x. BMC Health Serv Res. 2023. PMID: 37674143 Free PMC article.
-
Continuity of care in diverse ethnic groups: a general practice record study in England.Br J Gen Pract. 2023 Mar 30;73(729):e257-e266. doi: 10.3399/BJGP.2022.0271. Print 2023 Apr. Br J Gen Pract. 2023. PMID: 36316161 Free PMC article.
-
Continuity of care in primary healthcare settings among patients with chronic diseases in Saudi Arabia.SAGE Open Med. 2023 Oct 29;11:20503121231208648. doi: 10.1177/20503121231208648. eCollection 2023. SAGE Open Med. 2023. PMID: 37915839 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
