

Non-maintenance intravesical Bacillus Calmette-Guérin induction therapy with eight doses in patients with high- or highest-risk non-muscle invasive bladder cancer: a retrospective non-randomized comparative study
- PMID: 33706705
- PMCID: PMC7948348
- DOI: 10.1186/s12885-021-07966-7
Non-maintenance intravesical Bacillus Calmette-Guérin induction therapy with eight doses in patients with high- or highest-risk non-muscle invasive bladder cancer: a retrospective non-randomized comparative study
Abstract
Background: To explore possible solutions to overcome chronic Bacillus Calmette-Guérin (BCG) shortage affecting seriously the management of non-muscle invasive bladder cancer (NMIBC) in Europe and throughout the world, we investigated whether non-maintenance eight-dose induction BCG (iBCG) was comparable to six-dose iBCG plus maintenance BCG (mBCG).
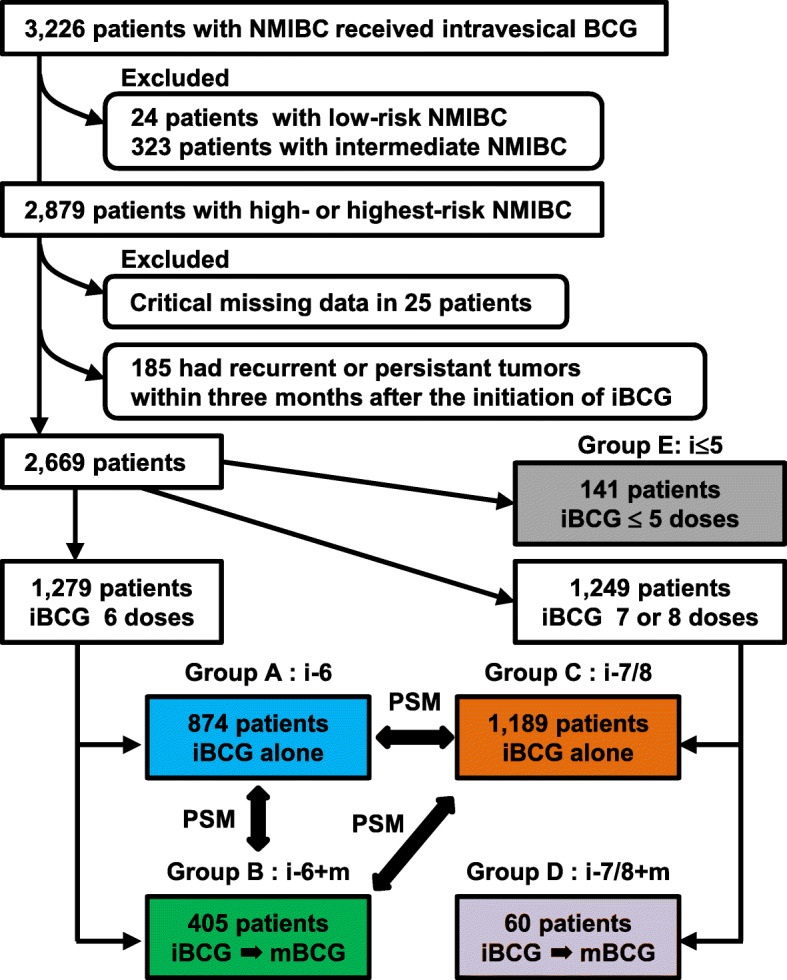
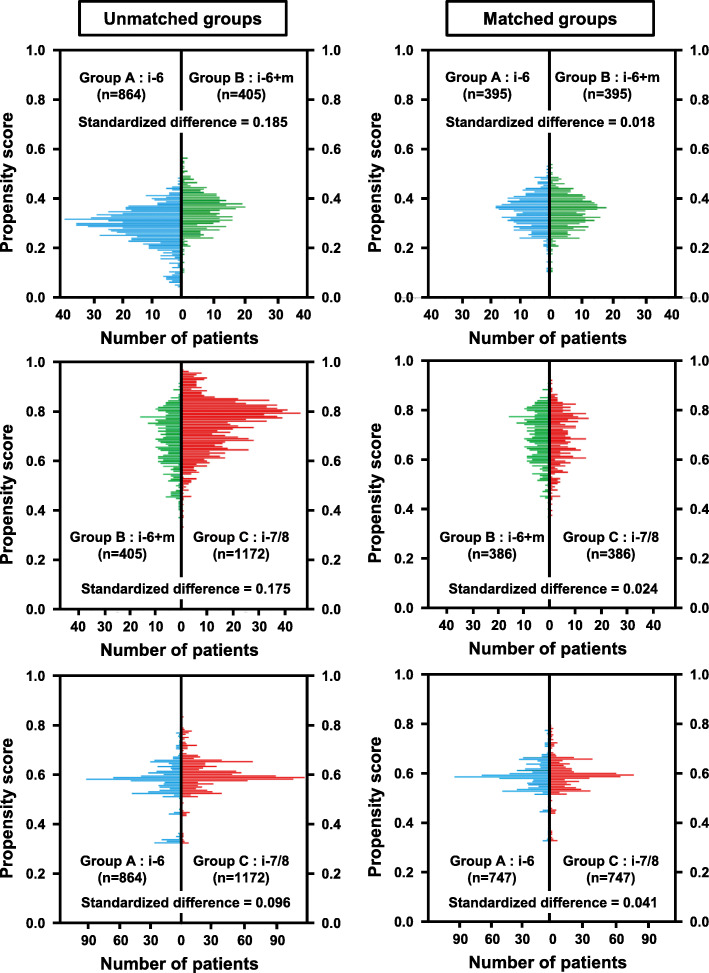
Methods: This observational study evaluated 2669 patients with high- or highest-risk NMIBC who treated with iBCG with or without mBCG during 2000-2019. The patients were classified into five groups according to treatment pattern: 874 (33%) received non-maintenance six-dose iBCG (Group A), 405 (15%) received six-dose iBCG plus mBCG (Group B), 1189 (44%) received non-maintenance seven-/eight-dose iBCG (Group C), 60 (2.2%) received seven-/eight-dose iBCG plus mBCG, and 141 (5.3%) received only ≤5-dose iBCG. Recurrence-free survival (RFS), progression-free survival, and cancer-specific survival were estimated and compared using Kaplan-Meier analysis and the log-rank test, respectively. Propensity score-based one-to-one matching was performed using a multivariable logistic regression model based on covariates to obtain balanced groups. To eliminate possible immortal bias, 6-, 12-, 18-, and 24-month conditional landmark analyses of RFS were performed.
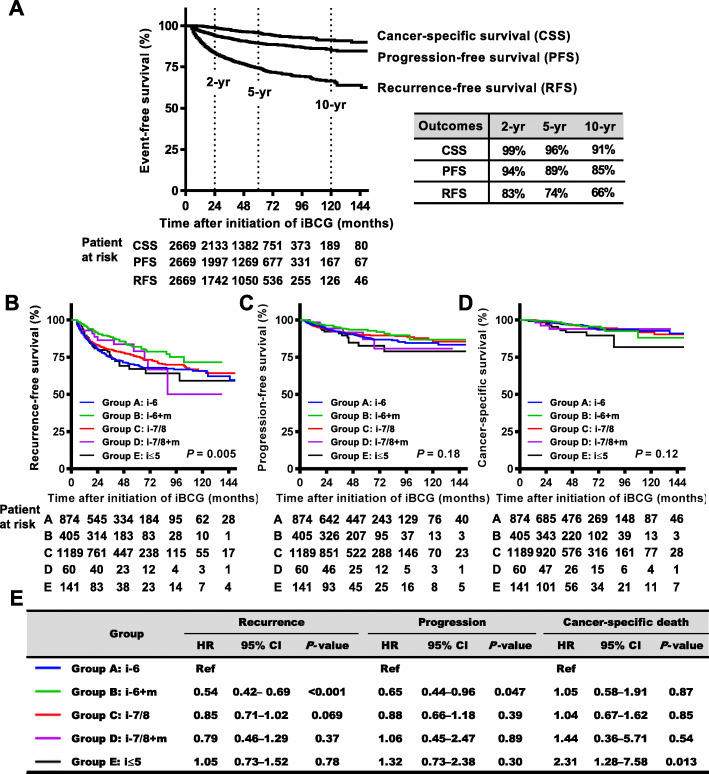
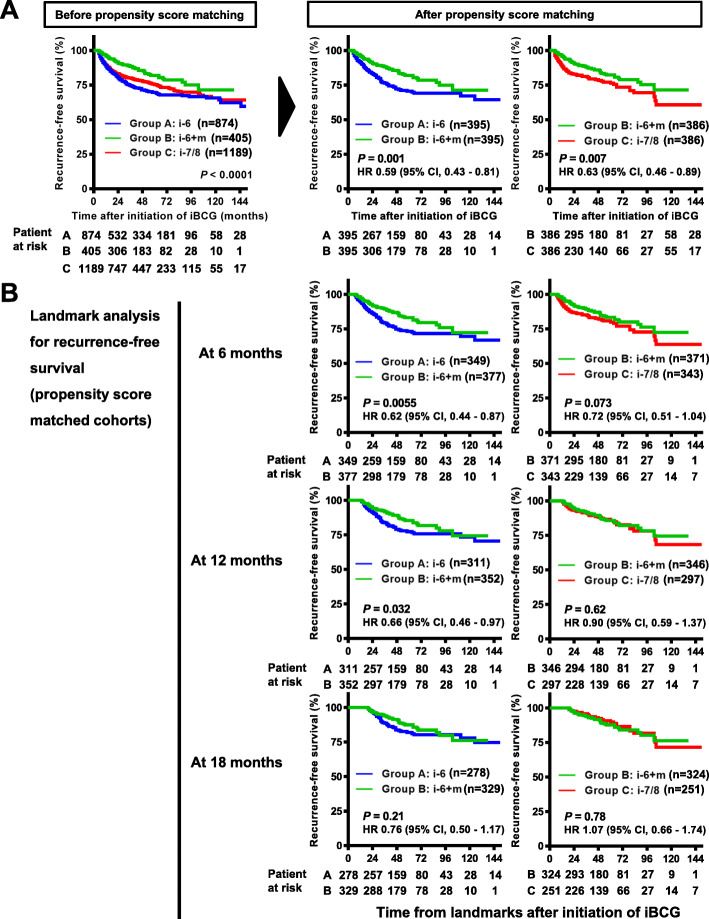
Results: RFS comparison confirmed that mBCG yielded significant benefit following six-dose iBCG (Group B) in recurrence risk reduction compared to iBCG alone (groups A and C) before (P < 0.001 and P = 0.0016, respectively) and after propensity score matching (P = 0.001 and P = 0.0074, respectively). Propensity score-matched sequential landmark analyses revealed no significant differences between groups B and C at 12, 18, and 24 months, whereas landmark analyses at 6 and 12 months showed a benefit of mBCG following six-dose iBCG compared to non-maintenance six-dose iBCG (P = 0.0055 and P = 0.032, respectively). There were no significant differences in the risks of progression and cancer-specific death in all comparisons of the matched cohorts.
Conclusions: Although non-maintenance eight-dose iBCG was inferior to six-dose iBCG plus mBCG, the former might be an alternative remedy in the BCG shortage era. To overcome this challenge, further investigation is warranted to confirm the real clinical value of non-maintenance eight-dose iBCG.
Keywords: Bacillus Calmette-Guérin (BCG); Intravesical therapy; Landmark analysis; Non-muscle invasive bladder cancer; Propensity score matching; Urinary bladder neoplasms.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Miyake M, Gotoh D, Shimada K, et al. Exploration of risk factors predicting outcomes for primary T1 high-grade bladder cancer and validation of the Spanish urological Club for Oncological Treatment scoring model: long-term follow-up experience at a single institute. Int J Urol. 2015;22:541–547. doi: 10.1111/iju.12749. - DOI - PubMed
-
- Matsumoto H, Shiraishi K, Azuma H, et al. Clinical practice guidelines for bladder Cancer 2019 update by the Japanese urological association: summary of the revision. Int J Urol. 2020. 10.1111/iju.14281 Online ahead of print. - PubMed
-
- Chen S, Zhang N, Shao J, Wang X. Maintenance versus non-maintenance intravesical Bacillus Calmette-Guerin instillation for non-muscle invasive bladder cancer: a systematic review and meta-analysis of randomized clinical trials. Int J Surg. 2018;52:248–257. doi: 10.1016/j.ijsu.2018.02.045. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
