

UK prevalence of underlying conditions which increase the risk of severe COVID-19 disease: a point prevalence study using electronic health records
- PMID: 33706738
- PMCID: PMC7948667
- DOI: 10.1186/s12889-021-10427-2
UK prevalence of underlying conditions which increase the risk of severe COVID-19 disease: a point prevalence study using electronic health records
Abstract
Background: Characterising the size and distribution of the population at risk of severe COVID-19 is vital for effective policy and planning. Older age, and underlying health conditions, are associated with higher risk of death from COVID-19. This study aimed to describe the population at risk of severe COVID-19 due to underlying health conditions across the United Kingdom.
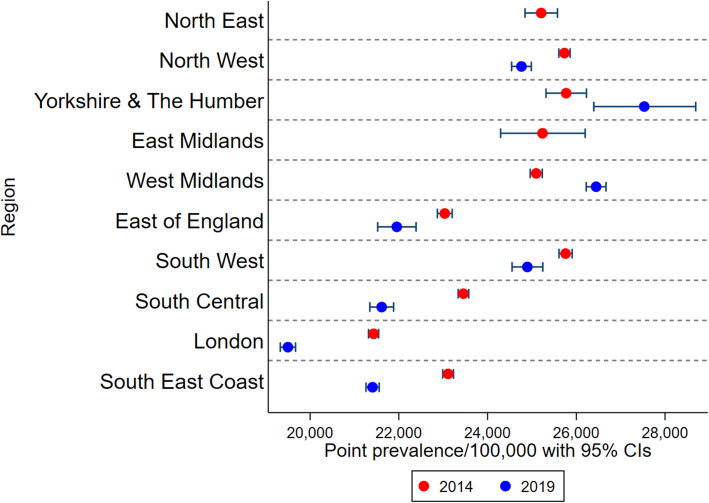
Methods: We used anonymised electronic health records from the Clinical Practice Research Datalink GOLD to estimate the point prevalence on 5 March 2019 of the at-risk population following national guidance. Prevalence for any risk condition and for each individual condition is given overall and stratified by age and region with binomial exact confidence intervals. We repeated the analysis on 5 March 2014 for full regional representation and to describe prevalence of underlying health conditions in pregnancy. We additionally described the population of cancer survivors, and assessed the value of linked secondary care records for ascertaining COVID-19 at-risk status.
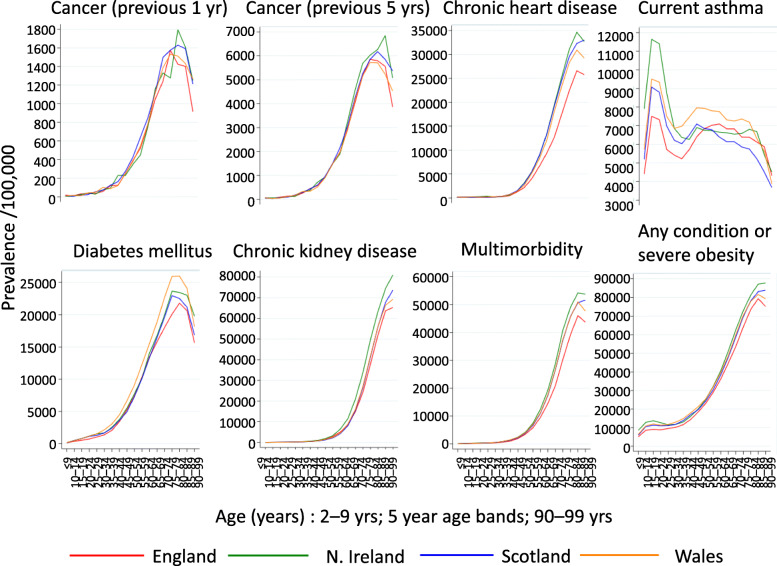
Results: On 5 March 2019, 24.4% of the UK population were at risk due to a record of at least one underlying health condition, including 8.3% of school-aged children, 19.6% of working-aged adults, and 66.2% of individuals aged 70 years or more. 7.1% of the population had multimorbidity. The size of the at-risk population was stable over time comparing 2014 to 2019, despite increases in chronic liver disease and diabetes and decreases in chronic kidney disease and current asthma. Separately, 1.6% of the population had a new diagnosis of cancer in the past 5 y.
Conclusions: The population at risk of severe COVID-19 (defined as either aged ≥70 years, or younger with an underlying health condition) comprises 18.5 million individuals in the UK, including a considerable proportion of school-aged and working-aged individuals. Our national estimates broadly support the use of Global Burden of Disease modelled estimates in other countries. We provide age- and region- stratified prevalence for each condition to support effective modelling of public health interventions and planning of vaccine resource allocation. The high prevalence of health conditions among older age groups suggests that age-targeted vaccination strategies may efficiently target individuals at higher risk of severe COVID-19.
Keywords: COVID-19; Electronic health records; Prevalence; Risk factors; United Kingdom.
Conflict of interest statement
JLW, DJG, NA, JAS, LS, MR, HM received grants from the NIHR HPRU in Immunisation to support the submitted work. RME received grants from HDR UK (MR/S003975/1) and UK MRC (MC_PC 19065). JKQ reports grants and personal fees from AZ, grants from Asthma UK, grants and personal fees from BI, grants and personal fees from Bayer, grants and personal fees from Insmed, grants and personal fees from GSK, grants from The Health Foundation, grants from MRC, grants from British Lung Foundation, outside the submitted work; RM reports personal fees from AMGEN, outside the submitted work; JAS reports grants from National Institute for Health Research, during the conduct of the study; grants from MRC, grants from Wellcome Trust, grants from GAVI The Vaccine Alliance, grants from Bill & Melinda Gates Foundation, outside the submitted work; LS reports grants from Wellcome, grants from MRC, grants from NIHR, grants from GSK, grants from BHF, grants from Diabetes UK, outside the submitted work; and Is a Trustee of the British Heart Foundation. The PHE Immunisation and Countermeasures Department provides vaccine manufacturers with post-marketing surveillance reports which the companies are required to submit to the UK Licensing authority in compliance with their Risk Management Strategy. A cost recovery charge is made for these reports.
Figures
References
-
- O'Driscoll M, Ribeiro Dos Santos G, Wang L, Cummings DAT, Azman AS, Paireau J, Fontanet A, Cauchemez S, Salje H. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature. 2021;590(7844):140–5. - PubMed
-
- Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, Curtis HJ, Mehrkar A, Evans D, Inglesby P, Cockburn J, McDonald HI, MacKenna B, Tomlinson L, Douglas IJ, Rentsch CT, Mathur R, Wong AYS, Grieve R, Harrison D, Forbes H, Schultze A, Croker R, Parry J, Hester F, Harper S, Perera R, Evans SJW, Smeeth L, Goldacre B. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584(7821):430–6. - PMC - PubMed
-
- de Lusignan S, Dorward J, Correa A, Jones N, Akinyemi O, Amirthalingam G, Andrews N, Byford R, Dabrera G, Elliot A, Ellis J, Ferreira F, Lopez Bernal J, Okusi C, Ramsay M, Sherlock J, Smith G, Williams J, Howsam G, Zambon M, Joy M, Hobbs FDR. Risk factors for SARS-CoV-2 among patients in the Oxford Royal College of General Practitioners Research and Surveillance Centre primary care network: a cross-sectional study. Lancet Infect Dis. 2020;20(9):1034–42. - PMC - PubMed
-
- Clift AK, Coupland CAC, Keogh RH, Diaz-Ordaz K, Williamson E, Harrison EM, et al. Living risk prediction algorithm (QCOVID) for risk of hospital admission and mortality from coronavirus 19 in adults: national derivation and validation cohort study. BMJ. 2020;371:m3731. doi: 10.1136/bmj.m3731. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
