

Predicting Disease Recurrence, Early Progression, and Overall Survival Following Surgical Resection for High-risk Localized and Locally Advanced Renal Cell Carcinoma
- PMID: 33707112
- PMCID: PMC8627688
- DOI: 10.1016/j.eururo.2021.02.025
Predicting Disease Recurrence, Early Progression, and Overall Survival Following Surgical Resection for High-risk Localized and Locally Advanced Renal Cell Carcinoma
Abstract
Background: Risk stratification for localized renal cell carcinoma (RCC) relies heavily on retrospective models, limiting their generalizability to contemporary cohorts.
Objective: To introduce a contemporary RCC prognostic model, developed using prospective, highly annotated data from a phase III adjuvant trial.
Design, setting, and participants: The model utilizes outcome data from the ECOG-ACRIN 2805 (ASSURE) RCC trial.
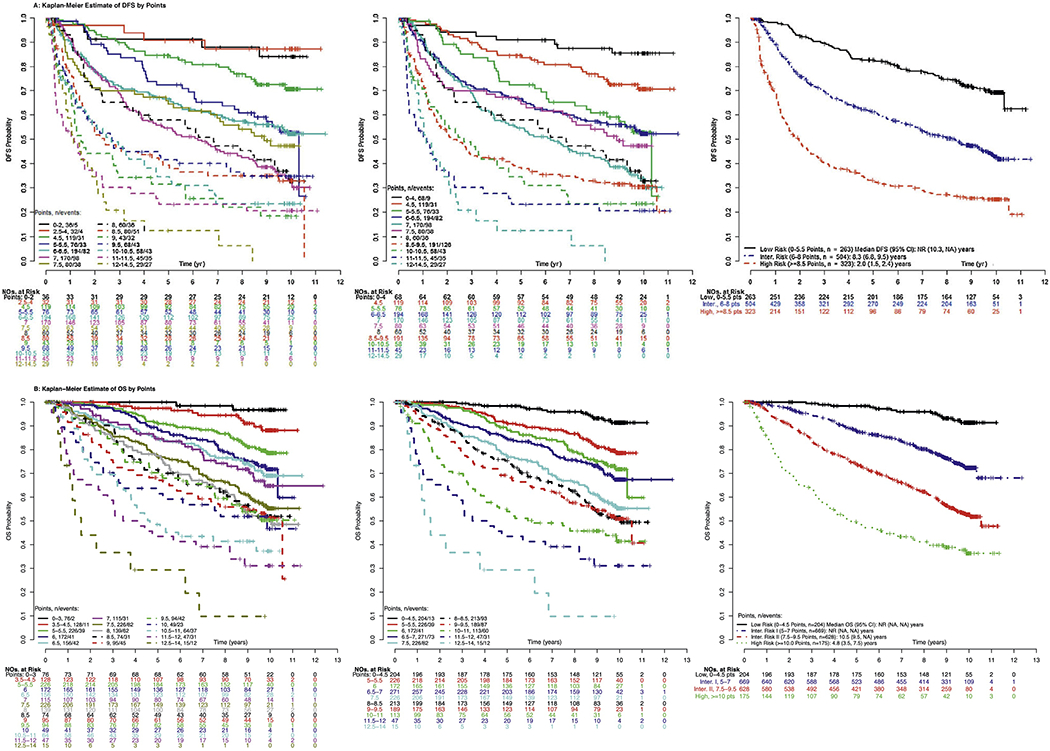
Outcome measurements and statistical analysis: The primary outcome for the model is disease-free survival (DFS), with overall survival (OS) and early disease progression (EDP) as secondary outcomes. Model performance was assessed using discrimination and calibration tests.
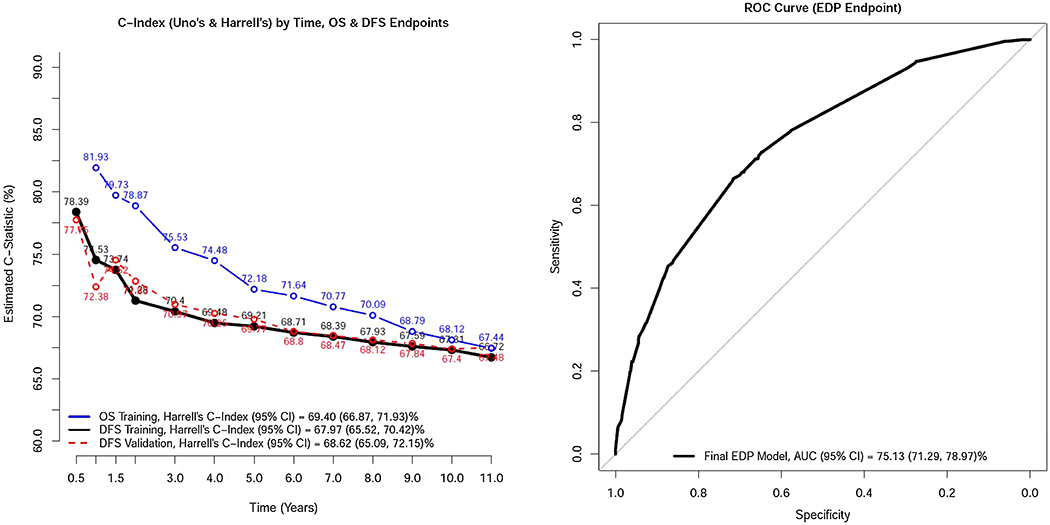
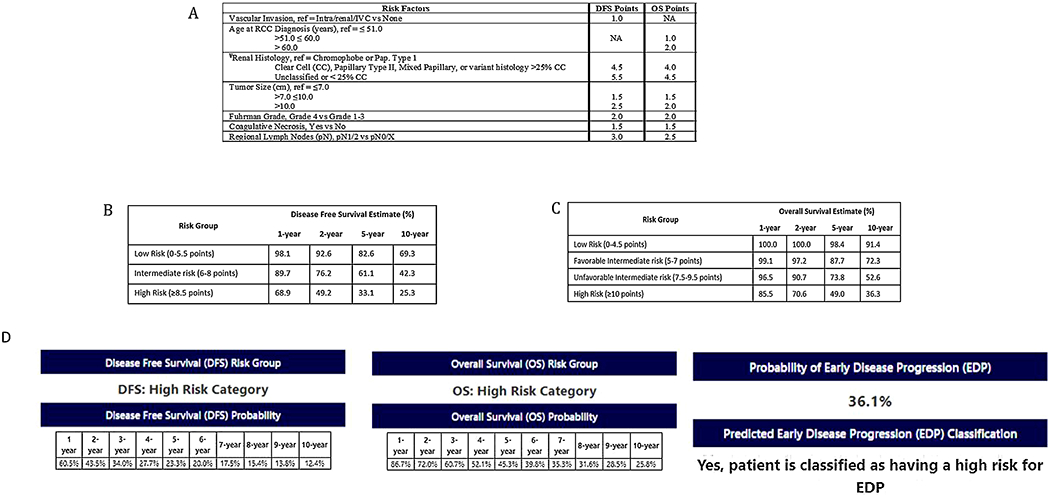
Results and limitations: A total of 1735 patients were included in the analysis, with 887 DFS events occurring over a median follow-up of 9.6 yr. Five common tumor variables (histology, size, grade, tumor necrosis, and nodal involvement) were included in each model. Tumor histology was the single most powerful predictor for each model outcome. The C-statistics at 1 yr were 78.4% and 81.9% for DFS and OS, respectively. Degradation of the DFS, DFS validation set, and OS model's discriminatory ability was seen over time, with a global c-index of 68.0% (95% confidence interval or CI [65.5, 70.4]), 68.6% [65.1%, 72.2%], and 69.4% (95% CI [66.9%, 71.9%], respectively. The EDP model had a c-index of 75.1% (95% CI [71.3, 79.0]).
Conclusions: We introduce a contemporary RCC recurrence model built and internally validated using prospective and highly annotated data from a clinical trial. Performance characteristics of the current model exceed available prognostic models with the added benefit of being histology inclusive and TNM agnostic.
Patient summary: Important decisions, including treatment protocols, clinical trial eligibility, and life planning, rest on our ability to predict cancer outcomes accurately. Here, we introduce a contemporary renal cell carcinoma prognostic model leveraging high-quality data from a clinical trial. The current model predicts three outcome measures commonly utilized in clinical practice and exceeds the predictive ability of available prognostic models.
Keywords: ASSURE trial; Disease-free survival; Prognostic model; Renal cell carcinoma.
Copyright © 2021 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Contemporary Prognostic Model for Renal Cell Carcinoma: Is it Time for Biomarkers?Eur Urol. 2021 Jul;80(1):32-33. doi: 10.1016/j.eururo.2021.04.019. Epub 2021 Apr 30. Eur Urol. 2021. PMID: 33934930 No abstract available.
-
Urological Oncology: Adrenal, Renal, Ureteral and Retroperitoneal Tumors.J Urol. 2021 Dec;206(6):1515-1517. doi: 10.1097/JU.0000000000002219. Epub 2021 Sep 9. J Urol. 2021. PMID: 34496608 No abstract available.
References
-
- American Joint Committee for Cancer Staging and End Results Reporting. Manual for staging of cancer. Chicago, IL: American Joint Committee; 1977.
-
- Kattan MW, Reuter V, Motzer RJ, Katz J, Russo P. A postoperative prognostic nomogram for renal cell carcinoma. J Urol 2001;166:63–7. - PubMed
-
- Sorbellini M, Kattan MW, Snyder ME, et al. A postoperative prognostic nomogram predicting recurrence for patients with conventional clear cell renal cell carcinoma. J Urol 2005;173:48–51. - PubMed
-
- Zisman A, Pantuck AJ, Wieder J, et al. Risk group assessment and clinical outcome algorithm to predict the natural history of patients with surgically resected renal cell carcinoma. J Clin Oncol 2002;20:4559–66. - PubMed
-
- Leibovich BC, Blute ML, Cheville JC, et al. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: a stratification tool for prospective clinical trials. Cancer 2003;97:1663–71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
