

Identification of Patients with CKD in Medical Databases: A Comparison of Different Algorithms
- PMID: 33707181
- PMCID: PMC8092062
- DOI: 10.2215/CJN.15691020
Identification of Patients with CKD in Medical Databases: A Comparison of Different Algorithms
Abstract
Background and objectives: Despite CKD consensus definitions, epidemiologic studies use multiple different algorithms to identify CKD. We aimed to elucidate if this affects the patient characteristics and the estimated prevalence and prognosis of CKD by applying six different algorithms to identify CKD in population-based medical databases and compare the cohorts.
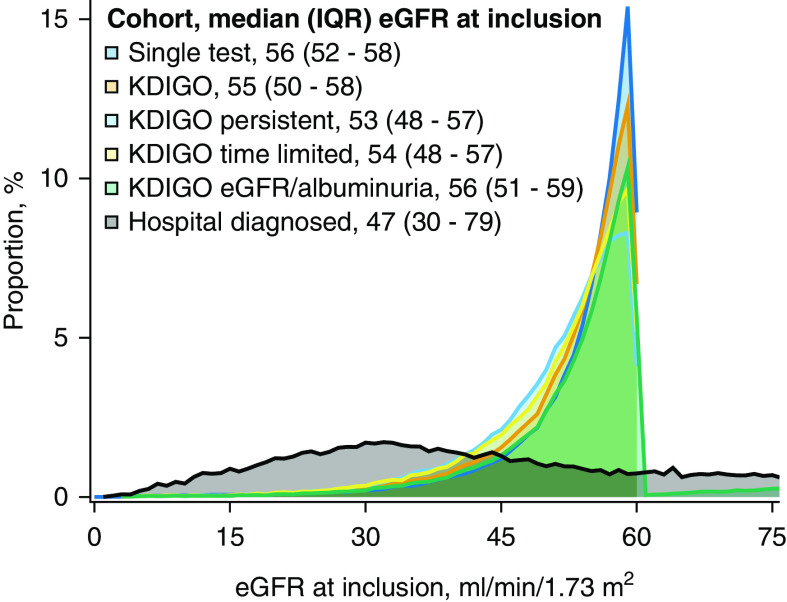
Design, setting, participants, & measurements: Patients with CKD in Northern Denmark (2009-2016) were identified using six different algorithms: five were laboratory based defined by (1) one measured outpatient eGFR <60 ml/min per 1.73 m2 (single test, n=103,435), (2) two such findings ≥90 days apart (Kidney Disease Improving Global Outcomes, n=84,688), (3) two such findings ≥90 days apart with no eGFR >60 ml/min per 1.73 m2 observed in-between (Kidney Disease Improving Global Outcomes, persistent, n=68,994), (4) two such findings ≥90 and <365 days apart (Kidney Disease Improving Global Outcomes, time limited, n=75,031), and (5) two eGFRs <60 ml/min per 1.73 m2 or two urine albumin-creatinine ratios >30 mg/g ≥90 days apart (Kidney Disease Improving Global Outcomes, eGFR/albuminuria, n=100,957). The sixth included patients identified by reported in- and outpatient hospital International Classification of Diseases diagnoses of CKD (hospital-diagnosed, n=27,947). For each cohort, we estimated baseline eGFR, CKD prevalence, and 1-year mortality using the Kaplan-Meier method.
Results: The five different laboratory-based algorithms resulted in large differences in the estimated prevalence of CKD from 4637-8327 per 100,000 population. In contrast, 1-year mortality varied only slightly (7%-9%). Baseline eGFR levels at diagnosis were comparable (53-56 ml/min per 1.73 m2), whereas median time since first recorded eGFR <60 ml/min per 1.73 m2 varied from 0 months (single-test) to 17 months (Kidney Disease Improving Global Outcomes, persistent). The hospital-diagnosed algorithm yielded markedly lower CKD prevalence (775 per 100,000 population), a lower baseline eGFR (47 ml/min per 1.73 m2), longer time since first eGFR <60 ml/min per 1.73 m2 (median 70 months), and much higher 1-year mortality (22%).
Conclusions: Population prevalence of CKD identified in medical databases greatly depends on the applied algorithm to define CKD. Despite these differences, laboratory-based algorithms produce cohorts with similar prognosis.
Podcast: This article contains a podcast at https://www.asn-online.org/media/podcast/CJASN/2021_03_11_CJN15691020_final.mp3.
Keywords: algorithms; chronic kidney disease; epidemiology; glomerular filtration rate; hospital records; incidence; mortality; prevalence; prognosis; registries.
Copyright © 2021 by the American Society of Nephrology.
Figures




References
-
- Eriksen BO, Ingebretsen OC: The progression of chronic kidney disease: A 10-year population-based study of the effects of gender and age. Kidney Int 69: 375–382, 2006 - PubMed
-
- Richards N, Harris K, Whitfield M, O’Donoghue D, Lewis R, Mansell M, Thomas S, Townend J, Eames M, Marcelli D: The impact of population-based identification of chronic kidney disease using estimated glomerular filtration rate (eGFR) reporting. Nephrol Dial Transplant 23: 556–561, 2008 - PubMed
-
- Stevens PE, de Lusignan S, Farmer CKT, Tomson CRV: Engaging primary care in CKD initiatives: The UK experience. Nephrol Dial Transplant 27[Suppl 3]: iii5–iii11, 2012 - PubMed
-
- John R, Webb M, Young A, Stevens PE: Unreferred chronic kidney disease: A longitudinal study. Am J Kidney Dis 43: 825–835, 2004 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
