

Tilsotolimod with Ipilimumab Drives Tumor Responses in Anti-PD-1 Refractory Melanoma
- PMID: 33707233
- PMCID: PMC8544022
- DOI: 10.1158/2159-8290.CD-20-1546
Tilsotolimod with Ipilimumab Drives Tumor Responses in Anti-PD-1 Refractory Melanoma
Abstract
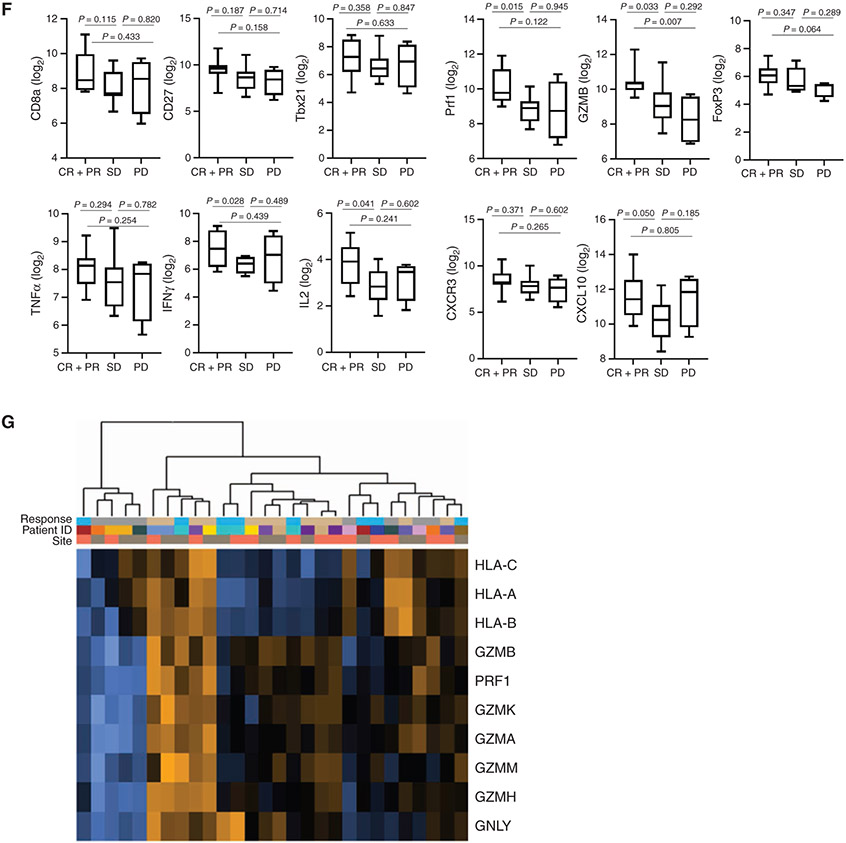
Many patients with advanced melanoma are resistant to immune checkpoint inhibition. In the ILLUMINATE-204 phase I/II trial, we assessed intratumoral tilsotolimod, an investigational Toll-like receptor 9 agonist, with systemic ipilimumab in patients with anti-PD-1- resistant advanced melanoma. In all patients, 48.4% experienced grade 3/4 treatment-emergent adverse events. The overall response rate at the recommended phase II dose of 8 mg was 22.4%, and an additional 49% of patients had stable disease. Responses in noninjected lesions and in patients expected to be resistant to ipilimumab monotherapy were observed. Rapid induction of a local IFNα gene signature, dendritic cell maturation and enhanced markers of antigen presentation, and T-cell clonal expansion correlated with clinical response. A phase III clinical trial with this combination (NCT03445533) is ongoing. SIGNIFICANCE: Despite recent developments in advanced melanoma therapies, most patients do not experience durable responses. Intratumoral tilsotolimod injection elicits a rapid, local type 1 IFN response and, in combination with ipilimumab, activates T cells to promote clinical activity, including in distant lesions and patients not expected to respond to ipilimumab alone.This article is highlighted in the In This Issue feature, p. 1861.
©2021 American Association for Cancer Research.
Figures






References
-
- Zimmer L, Apuri S, Eroglu Z, Kottschade LA, Forschner A, Gutzmer R, et al. Ipilimumab alone or in combination with nivolumab after progression on anti-PD-1 therapy in advanced melanoma. Eur J Cancer 2017;75:47–55. - PubMed
-
- Long GV, Robert C, Blank CU, Ribas A, Mortier L, Schachter J, et al. Outcomes in patients (pts) treated with ipilimumab (ipi) after pembrolizumab (pembro) in KEYNOTE-006. Pig Cell Mel Res 2017;30:118.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
