

Metabolomic analyses of COVID-19 patients unravel stage-dependent and prognostic biomarkers
- PMID: 33707411
- PMCID: PMC7948172
- DOI: 10.1038/s41419-021-03540-y
Metabolomic analyses of COVID-19 patients unravel stage-dependent and prognostic biomarkers
Erratum in
-
Correction: Metabolomic analyses of COVID-19 patients unravel stage-dependent and prognostic biomarkers.Cell Death Dis. 2024 Feb 14;15(2):142. doi: 10.1038/s41419-024-06519-7. Cell Death Dis. 2024. PMID: 38355585 Free PMC article. No abstract available.
Abstract
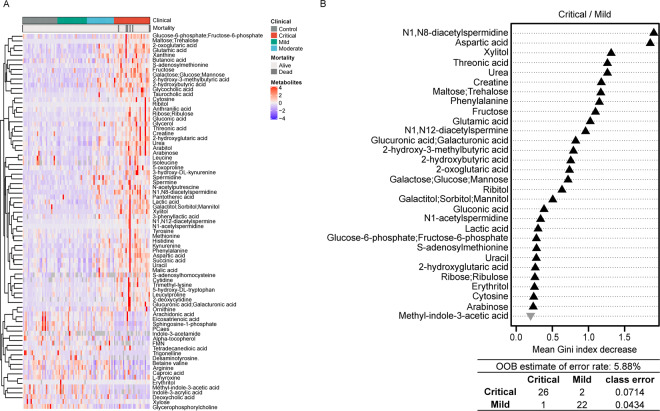
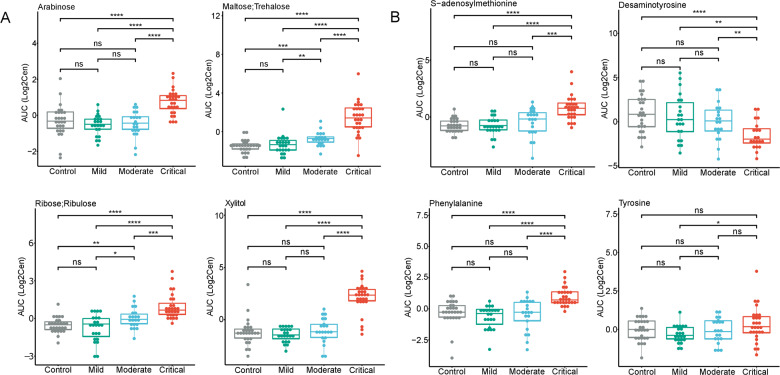
The circulating metabolome provides a snapshot of the physiological state of the organism responding to pathogenic challenges. Here we report alterations in the plasma metabolome reflecting the clinical presentation of COVID-19 patients with mild (ambulatory) diseases, moderate disease (radiologically confirmed pneumonitis, hospitalization and oxygen therapy), and critical disease (in intensive care). This analysis revealed major disease- and stage-associated shifts in the metabolome, meaning that at least 77 metabolites including amino acids, lipids, polyamines and sugars, as well as their derivatives, were altered in critical COVID-19 patient's plasma as compared to mild COVID-19 patients. Among a uniformly moderate cohort of patients who received tocilizumab, only 10 metabolites were different among individuals with a favorable evolution as compared to those who required transfer into the intensive care unit. The elevation of one single metabolite, anthranilic acid, had a poor prognostic value, correlating with the maintenance of high interleukin-10 and -18 levels. Given that products of the kynurenine pathway including anthranilic acid have immunosuppressive properties, we speculate on the therapeutic utility to inhibit the rate-limiting enzymes of this pathway including indoleamine 2,3-dioxygenase and tryptophan 2,3-dioxygenase.
Conflict of interest statement
G.K. has been holding research contracts with Bayer Healthcare, Daiichi Sankyo, Genentech, Glaxo Smyth Kline, Institut Mérieux, Kaleido, Lytix Pharma, Nucana, Oncolinx, PharmaMar, Samsara, Sotio, and Vasculox. G.K. is on the Board of Directors of the Bristol Myers Squibb Foundation France. G.K. is a scientific co-founder of everImmune, Samsara Therapeutics, and Therafast Bio. L.Z. is a founder of everImmune.
Figures




References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
