

Statins in High-Risk Chronic Obstructive Pulmonary Disease Outpatients: No Impact on Time to First Exacerbation and All-Cause Mortality - The STATUETTE Cohort Study
- PMID: 33707941
- PMCID: PMC7943323
- DOI: 10.2147/COPD.S296472
Statins in High-Risk Chronic Obstructive Pulmonary Disease Outpatients: No Impact on Time to First Exacerbation and All-Cause Mortality - The STATUETTE Cohort Study
Erratum in
-
Erratum: Statins in High-Risk Chronic Obstructive Pulmonary Disease Outpatients: No Impact on Time to First Exacerbation and All-Cause Mortality - The STATUETTE Cohort Study [Corrigendum].Int J Chron Obstruct Pulmon Dis. 2021 Aug 19;16:2393-2395. doi: 10.2147/COPD.S332259. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 34447246 Free PMC article.
Abstract
Background: Statins have, due to their anti-inflammatory properties, been suggested to potentially improve chronic obstructive pulmonary disease (COPD) outcomes. We aimed to investigate the effect of statins on time to first exacerbation and all-cause mortality in high-risk COPD outpatients.
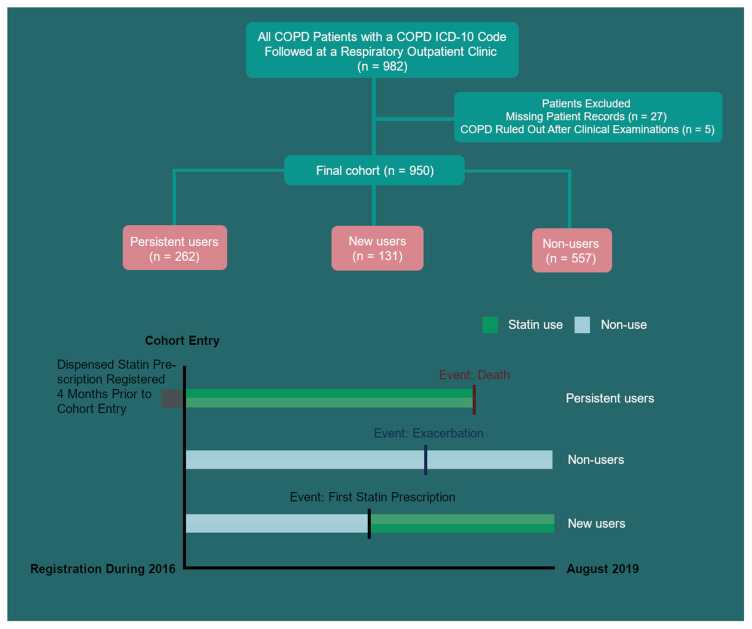
Methods: All outpatients with COPD seen at the Department of Respiratory Medicine, Copenhagen University Hospital Amager and Hvidovre, Denmark in 2016 were identified and followed for 3.5 years in this retrospective, registry-based cohort study of time to first acute exacerbation of COPD (AECOPD) or death. AECOPD was defined as a rescue course of oral corticosteroid and/or hospital admission. The association was estimated using time-varying crude and multivariable Cox proportional hazard regression.
Results: The cohort comprised 950 COPD outpatients, mean (SD) age 71 (11) years, and FEV1 44% predicted (IQR 33%; 57%). The annual exacerbation rate was 0.88 (1.68) and 211 patients (22%) had a history of hospital admission for AECOPD in the 12 months prior to index date. Three hundred and ninety-three patients (41.4%) were defined as statin users, with 131 (33.3%) having filled the first prescription for statin after index date. Statin use was not associated with reduced risk of AECOPD. When stratifying for moderate and severe exacerbations in a sub-analysis in the same model, statin use did not have an increased HR for exacerbation of either severity (HR = 1.02 (95% CI 0.85to 1.24; p = 0.811) and HR = 1.07 (95% CI 0.89 to 1.29; p = 0.492) respectively). Statin use was not associated with all-cause mortality (HR 1.05 (95% CI, 0.75 to 1.47, p = 0.777)).
Conclusion: We did not find any association between statin use and risk of AECOPD or all-cause mortality. The result adds to the evidence that an aggressive approach with statin treatment upfront is not beneficial in COPD, unless prescribed according to current guidelines for cardiovascular diseases.
Keywords: cardiovascular disease; chronic obstructive pulmonary disease; exacerbations; mortality; statins.
© 2021 Damkjær et al.
Conflict of interest statement
KH reports personal fees from TEVA, personal fees from AstraZeneca, personal fees from Chiesi, outside the submitted work; CSU reports personal fees from AstraZeneca, GSK, TEVA, Novartis, Chiesi, Boehringer-Ingelheim, SanofiGenzyme, ALK-Abello, MundiPharma, Orion Pharma and Actelion, outside the submitted work. NG reports personal fees from AstraZeneca, Boehringer-Ingelheim, Novartis and GSK, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
-
- The Lancet - Global Burden of Disease. Available from: https://www.thelancet.com/gbd. Accessed September13, 2020.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
