

Pathophysiology of heart failure
- PMID: 33708498
- PMCID: PMC7944197
- DOI: 10.21037/cdt-20-302
Pathophysiology of heart failure
Abstract
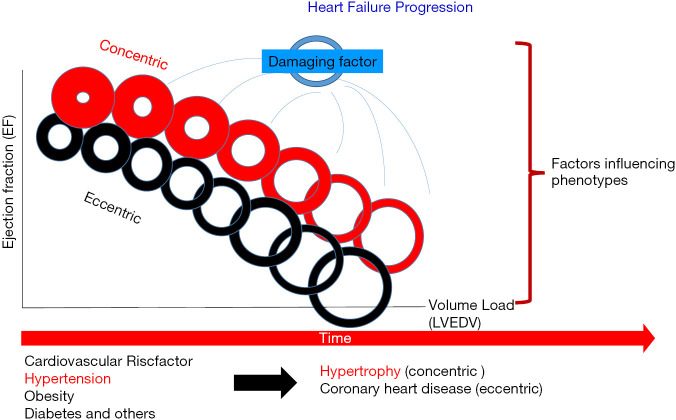
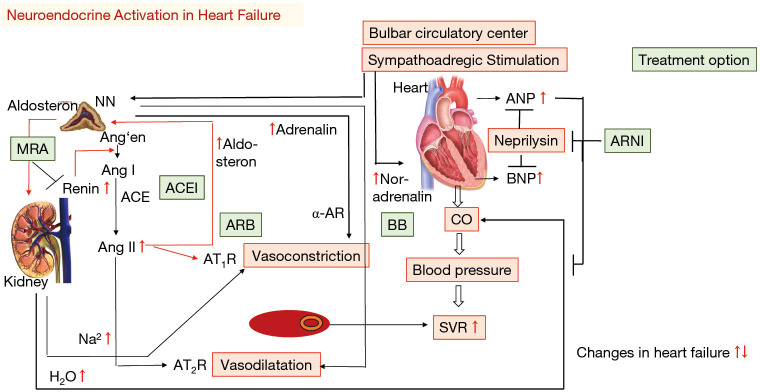
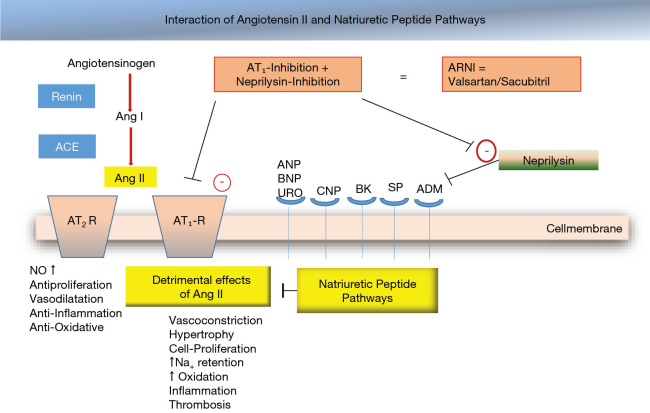
Heart failure is an epidemic disease which affects about 1% to 2% of the population worldwide. Both, the etiology and phenotype of heart failure differ largely. Following a cardiac injury (e.g., myocardial infarction, increased preload or afterload) cellular, structural and neurohumoral modulations occur that affect the phenotype being present. These processes influence the cell function among intra- as well as intercellular behavior. In consequence, activation of the sympathoadrenergic and renin-angiotensin-aldosterone-system takes place leading to adaptive mechanisms, which are accompanied by volume overload, tachycardia, dyspnoea and further deterioration of the cellular function (vicious circle). There exists no heart failure specific clinical sign; the clinical symptomatic shows progressive deterioration acutely or chronically. As a measure of cellular dysfunction, the level of neurohormones (norepinephrine) and natriuretic peptides (e.g., NT-pro BNP) increase. For the diagnosis of heart failure, noninvasive (echocardiography, NMR, NT-proBNP) and invasive (heart catheterization, biopsy) diagnostic procedures are implemented. Modulation of the activated systems by ß-blocker, ACE-inhibitors and ARNI improve outcome and symptoms in heart failure patients with left ventricular dysfunction. Interventional and surgical therapy options may be performed as well. The understanding of the underlying pathophysiology of heart failure is essential to initiate the adequate therapeutic option individually for each patient. Furthermore, prevention of cardiovascular risk factors is essential to lower the risk of heart failure.
Keywords: HFpEF; HFrEF; Heart failure; pathophysiology; treatment of heart failure.
2021 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The author has completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/cdt-20-302). The series “Heart Failure in the Young and Old: Insights into Various Therapies” was commissioned by the editorial office without any funding or sponsorship. The author has no other conflicts of interest to declare.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129-200. 10.1093/eurheartj/ehw128 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous