

Can the height of the parotid tumor be a predictor of malignancy?
- PMID: 33708554
- PMCID: PMC7944051
- DOI: 10.21037/gs-20-741
Can the height of the parotid tumor be a predictor of malignancy?
Abstract
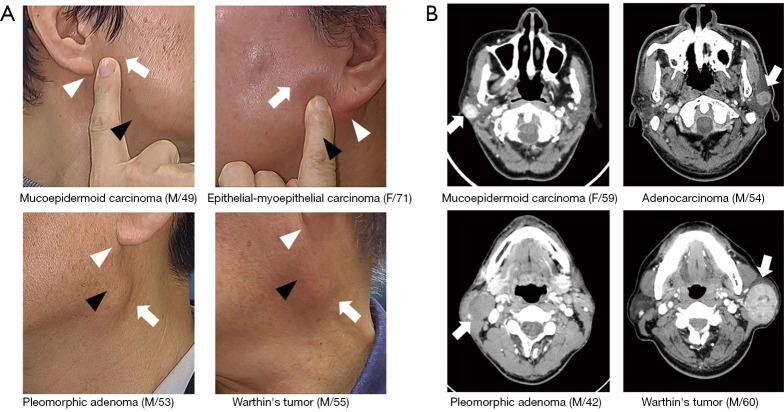
Background: Accurate diagnosis of malignancy in the parotid gland before surgery is often challenging. Various clues should be used to increase the index of suspicion for malignancy. We hypothesized that malignant lesions of the parotid gland are located at the superior part of the gland compared to benign ones.
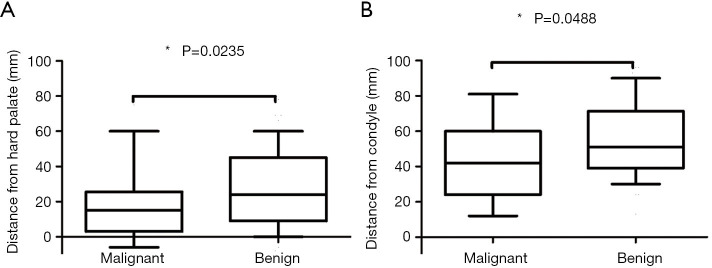
Methods: A total of 169 consecutive patients were included in this study whose medical records were retrospectively reviewed. Benign and malignant tumors were compared in size, height difference from five anatomical landmarks: hard palate, mastoid tip, earlobe, condylar head, and mandibular notch. The cutoff heights from significant landmarks (hard palate, condylar head) were estimated with ROC analysis and chi-square test.
Results: Twenty-nine patients (17.2%) were diagnosed with malignant and 140 patients (82.8%) as benign. The height differed significantly between benign and malignant tumors when the reference point was set for the hard palate (P=0.024) and the condylar head (P=0.049), with the cutoff height from reference points to be 22.5, 51.5 mm, respectively. Diagnostic values of parotid level difference presented higher sensitivity (75.9% for hard palate, 72.4% for condylar head vs. 47.8% for fine needle aspiration cytology) and lower false negative rate (24.1% for hard palate, 27.6% for condylar head vs. 52.2% for fine needle aspiration cytology) compared to fine needle aspiration cytology.
Conclusions: Malignant tumors of the parotid gland tend to locate at the superior part of the gland compared to benign tumors. Parotid tumors lying cephalad should raise an index of suspicion for malignancy. Height of the tumor in the parotid gland should be deliberately considered during the first encounter of the patient, which in turn could curate the next step in the diagnostic approach and treatment planning.
Keywords: Parotid neoplasm; physical examination; routine diagnostic test.
2021 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/gs-20-741). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources