

Establishing a prediction model of axillary nodal burden based on the combination of CT and ultrasound findings and the clinicopathological features in patients with early-stage breast cancer
- PMID: 33708557
- PMCID: PMC7944074
- DOI: 10.21037/gs-20-899
Establishing a prediction model of axillary nodal burden based on the combination of CT and ultrasound findings and the clinicopathological features in patients with early-stage breast cancer
Abstract
Background: Axillary lymph node (ALN) management in early-stage breast cancer (ESBC) patients has become less invasive during the past decades. Here, we tried to explore whether high nodal burden (HNB) in ESBC patients could be predicted preoperatively, so as to avoid unnecessary sentinel lymph node biopsy (SLNB).
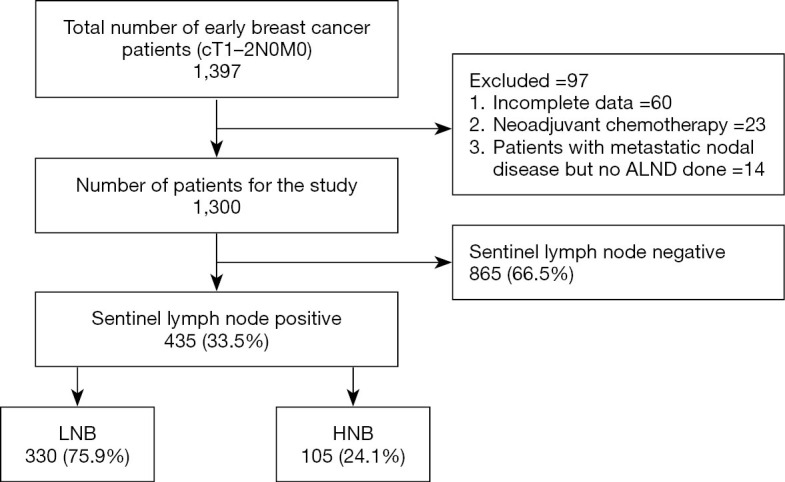
Methods: The clinicopathological and imaging data of patients with early invasive breast cancer (cT1-2N0M0) were analyzed retrospectively. Univariate and multivariate analyses were performed for the risk factors of axillary HNB in ESBC patients, and a risk prediction model of HNB was established.
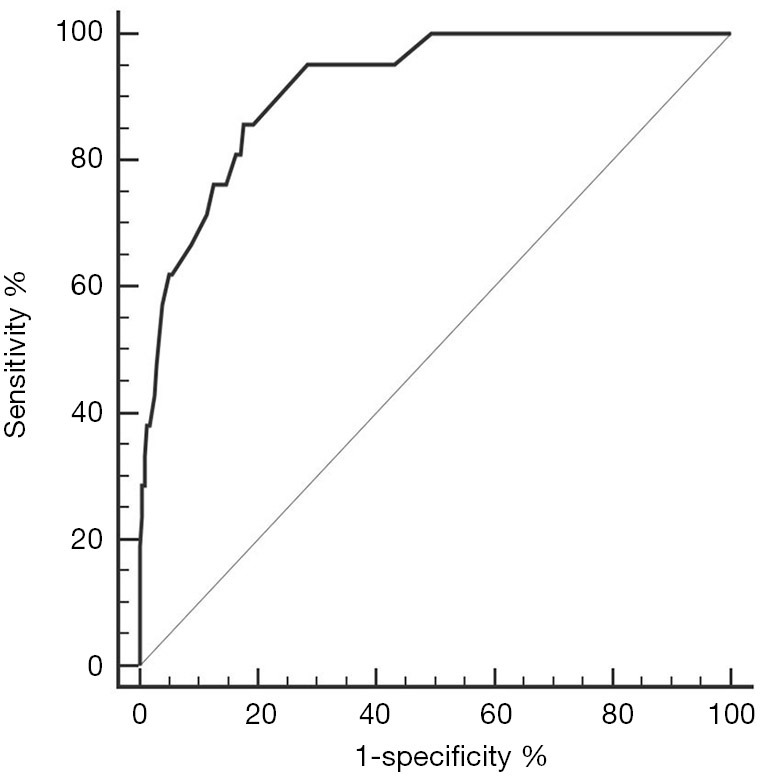
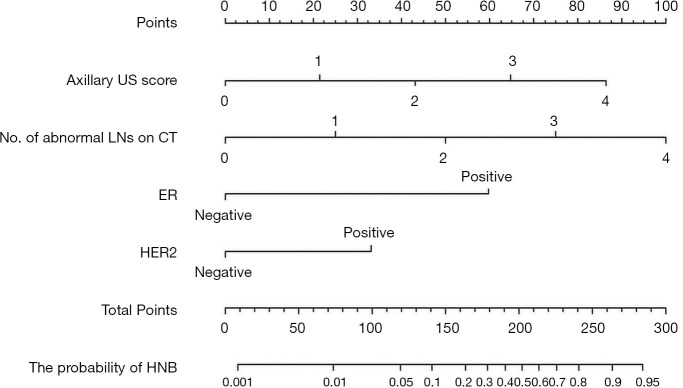
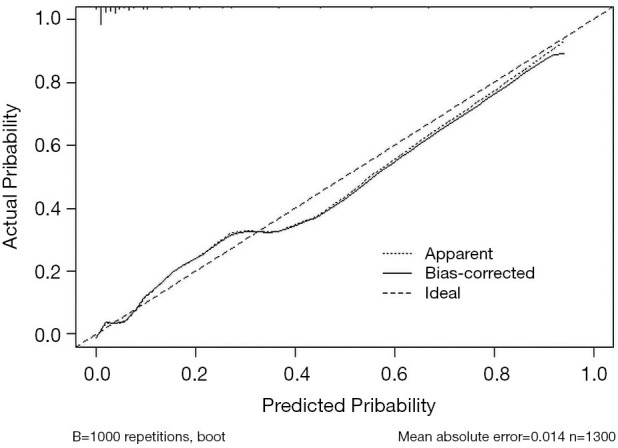
Results: HNB was identified in 105 (8.0%) of 1,300 ESBC patients. Multivariate analysis showed that estrogen receptors (ER) status, human epidermal growth factor receptor 2 (HER2) status, number of abnormal lymph nodes (LNs) on computed tomography (CT), and axillary score on ultrasound (US) were the risk factors of HNB (all P<0.05). The area under the receiver operating characteristic (ROC) curve in the prediction model was 0.914, with the sensitivity being 85.7% and the specificity being 82.4%. The calibration curve showed that the prediction model had good performance.
Conclusions: As a valuable tool for predicting HNB in ESBC patients, this newly established model helps clinicians to make reasonable axillary surgery decisions and thus avoid unnecessary SLNB.
Keywords: High nodal burden; axillary lymph node dissection (ALND); early-stage breast cancer (ESBC); sentinel lymph node (SLN).
2021 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/gs-20-899). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
[Establishment of a preoperative prediction model for axillary lymph node burden in patients with early breast cancer].Zhonghua Zhong Liu Za Zhi. 2021 May 23;43(5):563-568. doi: 10.3760/cma.j.cn112152-20200904-00796. Zhonghua Zhong Liu Za Zhi. 2021. PMID: 34034476 Chinese.
-
Determining Whether High Nodal Burden in Early Breast Cancer Patients Can Be Predicted Preoperatively to Avoid Sentinel Lymph Node Biopsy.J Breast Cancer. 2019 Mar;22(1):67-76. doi: 10.4048/jbc.2019.22.e8. J Breast Cancer. 2019. PMID: 30941234 Free PMC article.
-
Combining the Ultrasound Features of Primary Tumor and Axillary Lymph Nodes Can Reduce False-Negative Rate during the Prediction of High Axillary Node Burden in BI-RADS Category 4 or 5 Breast Cancer Lesions.Ultrasound Med Biol. 2020 Aug;46(8):1941-1948. doi: 10.1016/j.ultrasmedbio.2020.04.003. Epub 2020 May 22. Ultrasound Med Biol. 2020. PMID: 32451195
-
Breast cancer patients with a negative axillary ultrasound may have clinically significant nodal metastasis.Breast Cancer Res Treat. 2021 Jun;187(2):303-310. doi: 10.1007/s10549-021-06194-8. Epub 2021 Apr 10. Breast Cancer Res Treat. 2021. PMID: 33837870 Review.
-
Sentinel lymph node biopsy after previous axillary surgery: A review.Eur J Surg Oncol. 2012 Jan;38(1):8-15. doi: 10.1016/j.ejso.2011.10.003. Epub 2011 Oct 26. Eur J Surg Oncol. 2012. PMID: 22032909 Review.
Cited by
-
Multimodal Imaging of Target Detection Algorithm under Artificial Intelligence in the Diagnosis of Early Breast Cancer.J Healthc Eng. 2022 Jan 10;2022:9322937. doi: 10.1155/2022/9322937. eCollection 2022. J Healthc Eng. 2022. PMID: 35047160 Free PMC article.
-
Noninvasive Staging of Lymph Node Status in Breast Cancer Using Machine Learning: External Validation and Further Model Development.JMIR Cancer. 2023 Nov 20;9:e46474. doi: 10.2196/46474. JMIR Cancer. 2023. PMID: 37983068 Free PMC article.
References
-
- Krag DN, Anderson SJ, Julian TB, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol 2010;11:927-33. 10.1016/S1470-2045(10)70207-2 - DOI - PMC - PubMed
-
- Giuliano AE, Ballman KV, McCall L, et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA 2017;318:918-26. 10.1001/jama.2017.11470 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous