

Predictive risk factors for sentinel lymph node metastasis using preoperative contrast-enhanced ultrasound in early-stage breast cancer patients
- PMID: 33708558
- PMCID: PMC7944082
- DOI: 10.21037/gs-20-867
Predictive risk factors for sentinel lymph node metastasis using preoperative contrast-enhanced ultrasound in early-stage breast cancer patients
Abstract
Background: Sentinel lymph node biopsy (SLNB) is the standard procedure for axillary staging in clinically node-negative (cN0) breast cancer patients. The positive rate of SLNs in cN0 stage patients ranges from 20.5% to 25.5%, so identifying appropriate candidates for SLNB is quite challenging. The aims of this study were to assess whether contrast-enhanced ultrasound (CEUS) could be utilized to noninvasively predict SLN metastasis, and to explore the predictive value of the involved factors.
Methods: Between May 2016 and May 2018, 217 consenting breast cancer patients undergoing SLNB were enrolled. Before the surgery, CEUS was utilized to identify the SLNs, and predict whether metastasis had occurred according to their enhancement pattern. Blue dye was also used to identify the SLNs during SLNB. The rates of identification and accuracy of both methods were recorded. The predictive outcomes of SLNs identified by CEUS were recorded and compared with the pathological diagnosis.
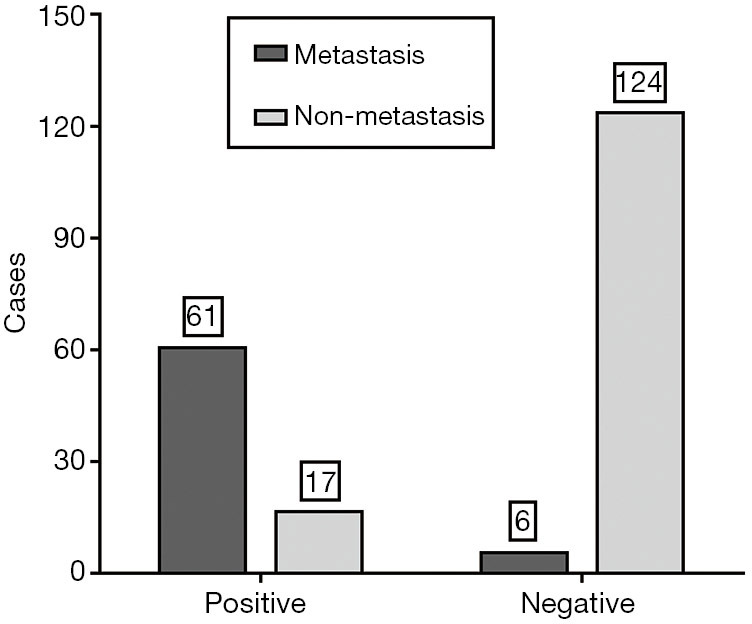
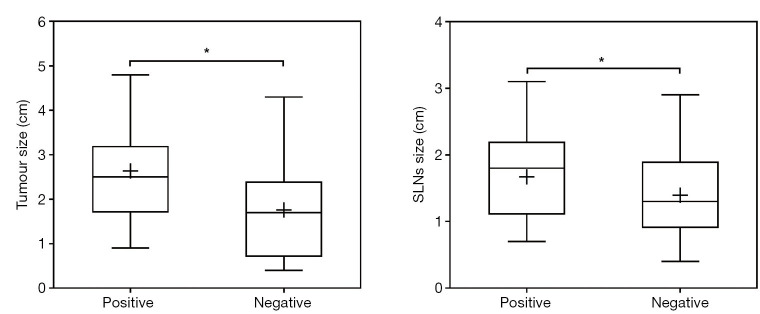
Results: Of the 217 cases, SLNs in 212 cases were successfully identified, comprising 208 cases identified by CEUS and 206 cases by blue dye, with no significant difference between the two methods (P=0.6470). A total of 78 cases were predicted SLN-positive preoperatively by CEUS, comprising 61 cases of SLN metastasis confirmed by pathology and 17 cases of no SLN metastasis, and 130 cases were predicted SLN-negative by CEUS, comprising 6 cases of SLN metastasis and 124 cases of no SLN metastasis. The sensitivity of CEUS preoperative prediction was 91.0%, the specificity was 87.9%, the positive and negative predictive values were 78.2% and 95.4%, respectively, and the accuracy was 88.9%. The maximum diameter size of positive SLNs predicted by CEUS was greater than that of negative SLNs (mean value 1.67±0.06 vs. 1.40±0.05 cm, P=0.0007). Similarly, the primary tumor size predicted SLN-positive by CEUS was greater than that in patients with negative SLNs (mean value 2.64±0.12 vs. 1.79±0.09 cm, P<0.0001).
Conclusions: CEUS accurately identified SLNs and can be used to noninvasively predict SLN metastasis in early-stage breast cancer patients. However, the primary tumor size and the SLN size should not be overlooked by clinicians when judging the status of SLNs. This novel method may be a recommended strategy for identifying appropriate SLNB candidates.
Keywords: Breast cancer; contrast-enhanced ultrasound (CEUS); sentinel lymph node (SLN); sentinel lymph node biopsy (SLNB).
2021 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/gs-20-867). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources