

Corneal Stromal Regeneration: A Review of Human Clinical Studies in Keratoconus Treatment
- PMID: 33708786
- PMCID: PMC7940685
- DOI: 10.3389/fmed.2021.650724
Corneal Stromal Regeneration: A Review of Human Clinical Studies in Keratoconus Treatment
Abstract
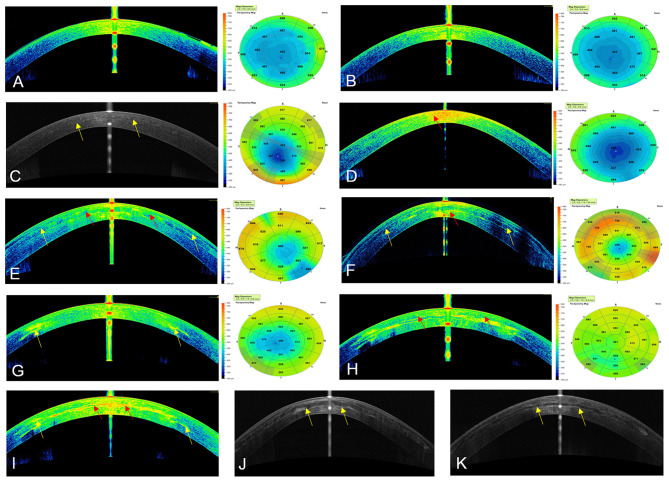
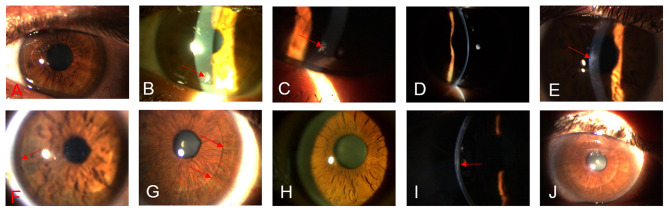
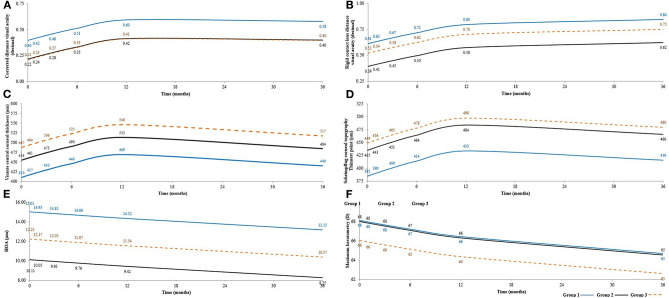
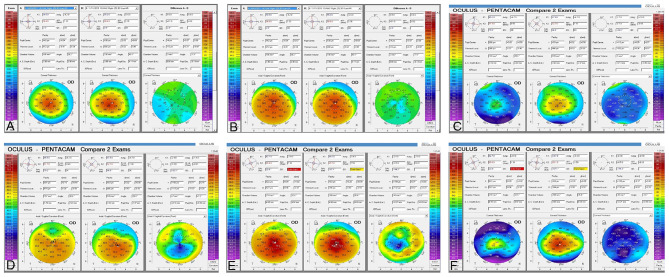
The use of advanced therapies with stem cells to reconstruct the complex tissue of corneal stroma has gained interest in recent years. Besides, collagen-based scaffolds bioengineering has been offered as another alternative over the last decade. The outcomes of the first clinical experience with stem cells therapy on corneal stroma regeneration in patients with advanced keratoconus were recently reported. Patients were distributed into three experimental groups: Group 1 (G-1) patients underwent implantation of autologous adipose-derived adult stem cells (ADASCs) alone, Group 2 (G-2) received a 120 μm decellularized donor corneal stromal laminas, and Group 3 (G-3) received a 120 μm recellularized donor laminas with ADASCs. A follow up of 36 months of clinical data, and 12 months of confocal microscopy study was performed, the authors found significant clinical improvement in almost all studied mean values of primary and secondary outcomes. Corneal confocal microscopy demonstrated an increase in cell density in the host stroma, as well as in the implanted tissue. Using different approaches, allogenic small incision lenticule extraction (SMILE) implantation was applied in cases with advanced keratoconus. Some authors reported the implantation of SMILE intrastromal lenticules combined with accelerated collagen cross-linking. Others performed intrastromal implantation of negative meniscus-shaped corneal stroma lenticules. Others have compared the outcomes of penetrating keratoplasty (PKP) vs. small-incision Intralase femtosecond (IFS) intracorneal concave lenticule implantation (SFII). Femtosecond laser-assisted small incision sutureless intrasotromal lamellar keratoplasty (SILK) has been also investigated. The published evidence shows that the implantation of autologous ADASCs, decellularized or recellularized human corneal stroma, allogenic SMILE lenticules corneal inlay, and recombinant cross-linked collagen have shown initially to be potentially effective for the treatment of advanced keratoconus. In light of the present evidence available, it can be said that the era of corneal stromal regeneration therapy has been already started.
Keywords: autologous adipose-derived adult stem cells; corneal bioengineering; corneal stem cell therapy; corneal surgery; cross-linked collagen; keratoconus; regenerative medicine; stem cells.
Copyright © 2021 El Zarif, Alió, Alió del Barrio, De Miguel, Abdul Jawad and Makdissy.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical