

Pegilodecakin as monotherapy or in combination with anti-PD-1 or tyrosine kinase inhibitor in heavily pretreated patients with advanced renal cell carcinoma: Final results of cohorts A, G, H and I of IVY Phase I study
- PMID: 33709428
- PMCID: PMC8251721
- DOI: 10.1002/ijc.33556
Pegilodecakin as monotherapy or in combination with anti-PD-1 or tyrosine kinase inhibitor in heavily pretreated patients with advanced renal cell carcinoma: Final results of cohorts A, G, H and I of IVY Phase I study
Abstract
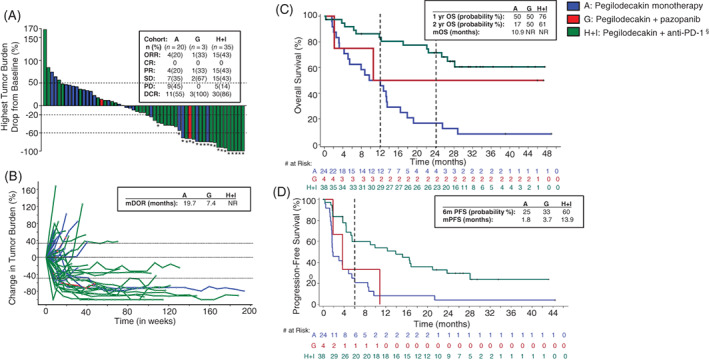
Interleukin (IL)-10 has anti-inflammatory and CD8+ T-cell-stimulating properties. Pegilodecakin (pegylated recombinant human IL-10) induces intratumoral antigen-specific CD8 + T-cells and upregulates IFNγ and major histocompatibility complexes (MHC) I and II. Pegilodecakin has single-agent activity with manageable toxicity in advanced renal cell carcinama (aRCC) (data cutoff 24 March 2016). Pegilodecakin with pembrolizumab or nivolumab revealed clinical activity in aRCC (data cutoff 1 July 2018). Here, we report for the first time the results of pegilodecakin+ pazopanib, and final results for monotherapy and long-term follow-up with pegilodecakin + anti-programmed cell death 1 (anti-PD-1) inhibitors (data cutoff 19 February 2019). Phase 1/1b multi-cohort dose escalation IVY study enrolled 353 patients. Sixty-six patients with aRCC were treated with pegilodecakin alone or with pazopanib or anti-PD-1 inhibitor in cohorts A, G, H and I (data cutoff 19 February 2019). Primary endpoints included safety and tolerability. Secondary endpoint was tumor response by immune-related response criteria (irRC). Pegilodecakin plus nivolumab or pembrolizumab yielded median progression-free survival (mPFS) of 13.9 months and 6-month PFS probability of 60%, 76% 1-year overall survival (OS) probability and 61% 2-year OS probability. Pegilodecakin monotherapy produced mPFS of 1.8 months, 6-month PFS probability 25%, 1-year OS 50%, and 2-year OS 17%. Median OS was not reached in both combinations. Objective response rates (ORRs) were 33% with pazopanib and 43% with anti-PD-1. Most common Grade 3/4 treatment-related adverse events included anemia, thrombocytopenia and hypertriglyceridemia. In these heavily pretreated renal cell carcinama cohorts of IVY, pegilodecakin+anti-PD-1 inhibitor showed promising clinical activity. Safety profile of pegilodecakin alone and with anti-PD-1 inhibitors was consistent as previously reported.
Keywords: nivolumab; pegilodecakin; pegylated IL-10; pembrolizumab; renal cancer.
© 2021 Eli Lilly and Company. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of Union for International Cancer Control.
Conflict of interest statement
The following represents disclosure information provided by the authors.
Figures
References
-
- Hasanov E, Gao J, Tannir NM. The immunotherapy revolution in kidney cancer treatment: scientific rationale and first‐generation results. Cancer J. 2020;26(5):419‐431. - PubMed
-
- Atkins MB, Tannir NM. Current and emerging therapies for first‐line treatment of metastatic clear cell renal cell carcinoma. Cancer Treat Rev. 2018;70:127‐137. - PubMed
-
- Chowdhury SMD, Voss MH, Hawkins RE, et al. A phase I/II study to assess the safety and efficacy of pazopanib (PAZ) and pembrolizumab (PEM) in patients (pts) with advanced renal cell carcinoma (aRCC). J Clin Oncol. 2017;35:4506.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
