

Prospective Validation of an Electronic Health Record-Based, Real-Time Suicide Risk Model
- PMID: 33710291
- PMCID: PMC7955273
- DOI: 10.1001/jamanetworkopen.2021.1428
Prospective Validation of an Electronic Health Record-Based, Real-Time Suicide Risk Model
Abstract
Importance: Numerous prognostic models of suicide risk have been published, but few have been implemented outside of integrated managed care systems.
Objective: To evaluate performance of a suicide attempt risk prediction model implemented in a vendor-supplied electronic health record to predict subsequent (1) suicidal ideation and (2) suicide attempt.
Design, setting, and participants: This observational cohort study evaluated implementation of a suicide attempt prediction model in live clinical systems without alerting. The cohort comprised patients seen for any reason in adult inpatient, emergency department, and ambulatory surgery settings at an academic medical center in the mid-South from June 2019 to April 2020.
Main outcomes and measures: Primary measures assessed external, prospective, and concurrent validity. Manual medical record validation of coded suicide attempts confirmed incident behaviors with intent to die. Subgroup analyses were performed based on demographic characteristics, relevant clinical context/setting, and presence or absence of universal screening. Performance was evaluated using discrimination (number needed to screen, C statistics, positive/negative predictive values) and calibration (Spiegelhalter z statistic). Recalibration was performed with logistic calibration.
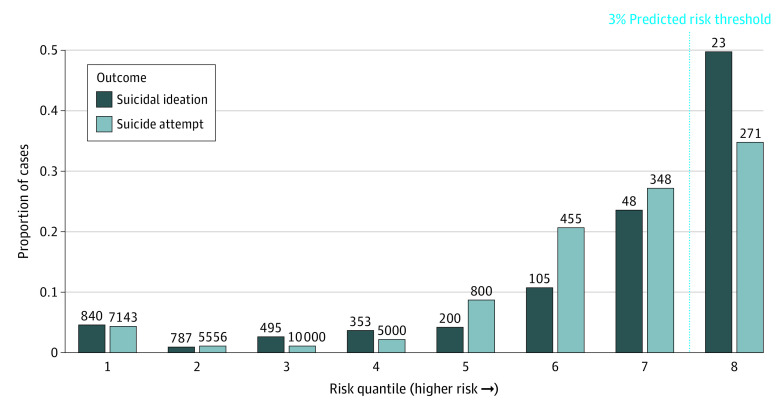
Results: The system generated 115 905 predictions for 77 973 patients (42 490 [54%] men, 35 404 [45%] women, 60 586 [78%] White, 12 620 [16%] Black). Numbers needed to screen in highest risk quantiles were 23 and 271 for suicidal ideation and attempt, respectively. Performance was maintained across demographic subgroups. Numbers needed to screen for suicide attempt by sex were 256 for men and 323 for women; and by race: 373, 176, and 407 for White, Black, and non-White/non-Black patients, respectively. Model C statistics were, across the health system: 0.836 (95% CI, 0.836-0.837); adult hospital: 0.77 (95% CI, 0.77-0.772); emergency department: 0.778 (95% CI, 0.777-0.778); psychiatry inpatient settings: 0.634 (95% CI, 0.633-0.636). Predictions were initially miscalibrated (Spiegelhalter z = -3.1; P = .001) with improvement after recalibration (Spiegelhalter z = 1.1; P = .26).
Conclusions and relevance: In this study, this real-time predictive model of suicide attempt risk showed reasonable numbers needed to screen in nonpsychiatric specialty settings in a large clinical system. Assuming that research-valid models will translate without performing this type of analysis risks inaccuracy in clinical practice, misclassification of risk, wasted effort, and missed opportunity to correct and prevent such problems. The next step is careful pairing with low-cost, low-harm preventive strategies in a pragmatic trial of effectiveness in preventing future suicidality.
Conflict of interest statement
Figures
Similar articles
-
Integration of Face-to-Face Screening With Real-time Machine Learning to Predict Risk of Suicide Among Adults.JAMA Netw Open. 2022 May 2;5(5):e2212095. doi: 10.1001/jamanetworkopen.2022.12095. JAMA Netw Open. 2022. PMID: 35560048 Free PMC article.
-
Clinician Suicide Risk Assessment for Prediction of Suicide Attempt in a Large Health Care System.JAMA Psychiatry. 2025 Jun 1;82(6):599-608. doi: 10.1001/jamapsychiatry.2025.0325. JAMA Psychiatry. 2025. PMID: 40202745
-
External Validation and Updating of a Statistical Civilian-Based Suicide Risk Model in US Naval Primary Care.JAMA Netw Open. 2023 Nov 1;6(11):e2342750. doi: 10.1001/jamanetworkopen.2023.42750. JAMA Netw Open. 2023. PMID: 37938841 Free PMC article.
-
Association Between Atopic Dermatitis and Suicidality: A Systematic Review and Meta-analysis.JAMA Dermatol. 2019 Feb 1;155(2):178-187. doi: 10.1001/jamadermatol.2018.4566. JAMA Dermatol. 2019. PMID: 30540348 Free PMC article.
-
Suicidal ideation and behaviors among women veterans with recent exposure to intimate partner violence.Gen Hosp Psychiatry. 2018 Nov-Dec;55:60-64. doi: 10.1016/j.genhosppsych.2018.10.006. Epub 2018 Oct 23. Gen Hosp Psychiatry. 2018. PMID: 30412860 Review.
Cited by
-
Scalable incident detection via natural language processing and probabilistic language models.Sci Rep. 2024 Oct 8;14(1):23429. doi: 10.1038/s41598-024-72756-7. Sci Rep. 2024. PMID: 39379449 Free PMC article.
-
Clinical Risk Prediction Models with Meta-Learning Prototypes of Patient Heterogeneity.Annu Int Conf IEEE Eng Med Biol Soc. 2023 Jul;2023:1-4. doi: 10.1109/EMBC40787.2023.10340765. Annu Int Conf IEEE Eng Med Biol Soc. 2023. PMID: 38083199 Free PMC article.
-
Improving ascertainment of suicidal ideation and suicide attempt with natural language processing.Sci Rep. 2022 Sep 7;12(1):15146. doi: 10.1038/s41598-022-19358-3. Sci Rep. 2022. PMID: 36071081 Free PMC article.
-
Developing a suicide risk model for use in the Indian Health Service.Npj Ment Health Res. 2024 Oct 16;3(1):47. doi: 10.1038/s44184-024-00088-5. Npj Ment Health Res. 2024. PMID: 39414996 Free PMC article.
-
Integration of Face-to-Face Screening With Real-time Machine Learning to Predict Risk of Suicide Among Adults.JAMA Netw Open. 2022 May 2;5(5):e2212095. doi: 10.1001/jamanetworkopen.2022.12095. JAMA Netw Open. 2022. PMID: 35560048 Free PMC article.
References
-
- World Health Organization . Suicide in the world: global health estimates. Published September 9, 2019. Accessed February 8, 2021. https://www.who.int/publications/i/item/suicide-in-the-world
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
