

An Overview of PARP Inhibitors for the Treatment of Breast Cancer
- PMID: 33710534
- PMCID: PMC8105250
- DOI: 10.1007/s11523-021-00796-4
An Overview of PARP Inhibitors for the Treatment of Breast Cancer
Abstract
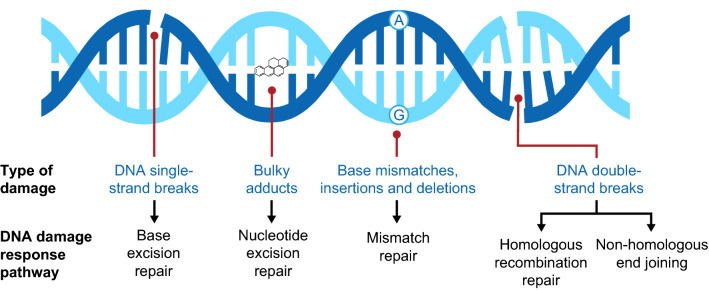
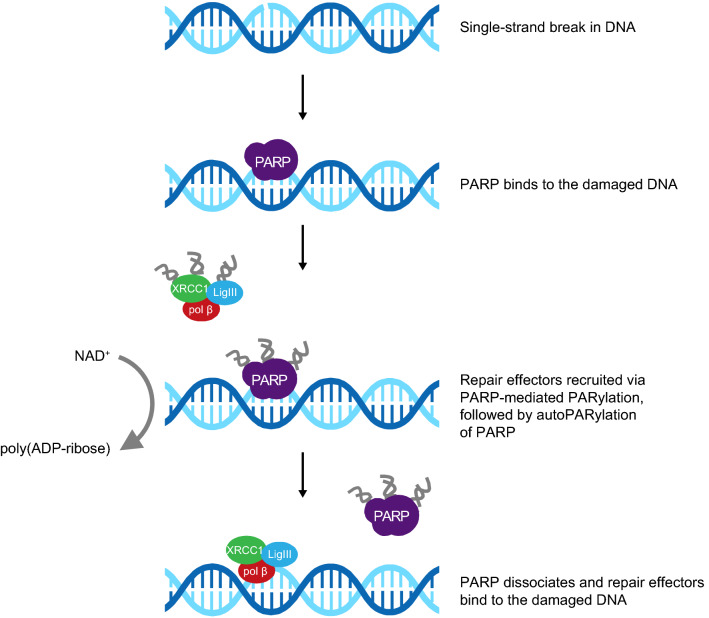
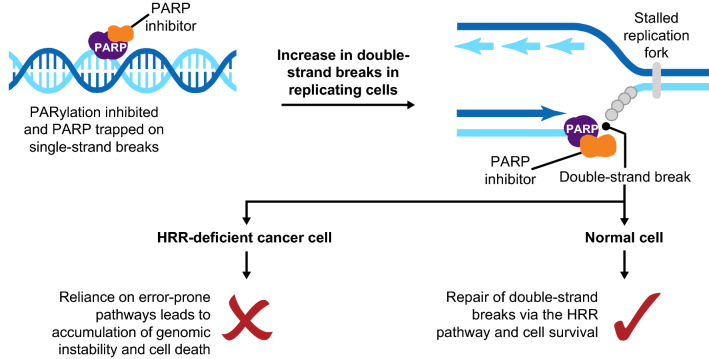
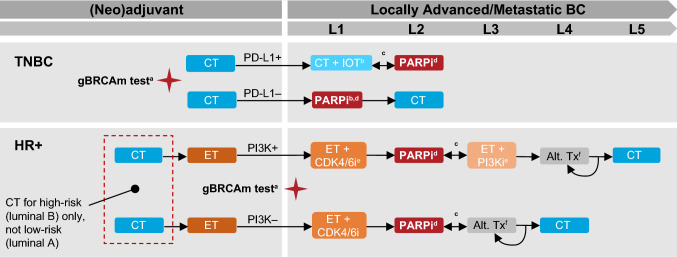
Loss-of-function mutations in BRCA1 and BRCA2 are detected in at least 5% of unselected patients with breast cancer (BC). These BC susceptibility genes encode proteins critical for DNA homologous recombination repair (HRR). This review provides an update on oral poly(ADP-ribose) polymerase (PARP) inhibitors for the treatment of BC. Olaparib and talazoparib are PARP inhibitors approved as monotherapies for deleterious/suspected deleterious germline BRCA-mutated, HER2-negative BC. Olaparib is approved in the USA for metastatic BC and in Europe for locally advanced/metastatic BC. Talazoparib is approved for locally advanced/metastatic BC in the USA and Europe. In phase 3 trials, olaparib and talazoparib monotherapies demonstrated significant progression-free survival benefits compared with chemotherapy. Common toxicities were effectively managed by supportive treatment and dose interruptions/reductions. Veliparib combined with platinum-based chemotherapy has also shown promise for locally advanced/metastatic BC in a phase 3 trial. Differences in efficacy and safety across PARP inhibitors (olaparib, talazoparib, veliparib, niraparib, rucaparib) may relate to differences in potency of PARP trapping on DNA and cytotoxic specificity. PARP inhibitors are being investigated in early BC, in novel combinations, and in patients without germline BRCA mutations, including those with somatic BRCA mutations and other HRR gene mutations. Ongoing phase 2/3 studies include PARP inhibitors combined with immune checkpoint inhibitors for the treatment of triple-negative BC. Wider access to testing for BRCA and other mutations, and to genetic counseling, are required to identify patients who could benefit from PARP inhibitor therapy. The advent of PARP inhibitors has potential benefits for BC treatment beyond the locally advanced/metastatic setting.
Conflict of interest statement
Laura Cortesi reports honoraria from AstraZeneca, Merck Sharp & Dohme, and Pfizer, and consultancy for Pfizer, Novartis, Tesaro, and Clovis. Hope S. Rugo reports research support to the University of California San Francisco from Pfizer, Merck, Novartis, Lilly, Macrogenics, Roche, OBI, Odonate, Eisai, and Daichi, as well as travel support from Pfizer, Novartis, Roche, and Mylan. Christian Jackisch has received honoraria from Amgen, Celgene, Lilly, Novartis, Pfizer, AstraZeneca, and Roche, and research support from Genomic Health.
Figures
References
-
- Ferlay J, Colombet M, Soerjomataram I, Mathers C, Parkin DM, Pineros M, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144:1941–1953. - PubMed
-
- World Health Organization. Breast cancer. 2020. https://www.who.int/cancer/prevention/diagnosis-screening/breast-cancer/en/. Accessed 21 Sept 2020.
-
- Maajani K, Jalali A, Alipour S, Khodadost M, Tohidinik HR, Yazdani K. The global and regional survival rate of women with breast cancer: a systematic review and meta-analysis. Clin Breast Cancer. 2019;19:165–177. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
