

Painful and non-painful diabetic neuropathy, diagnostic challenges and implications for future management
- PMID: 33711103
- PMCID: PMC8320269
- DOI: 10.1093/brain/awab079
Painful and non-painful diabetic neuropathy, diagnostic challenges and implications for future management
Abstract
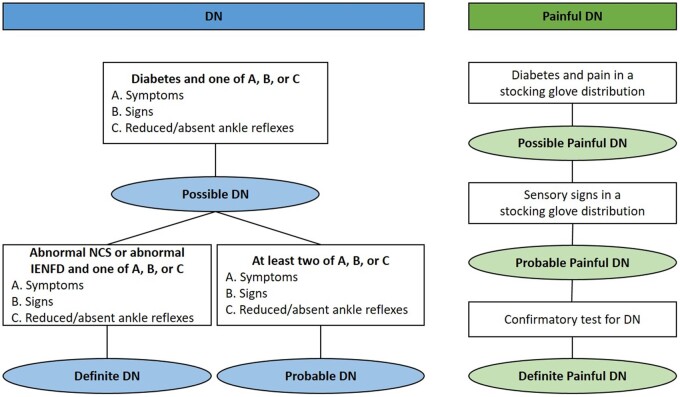
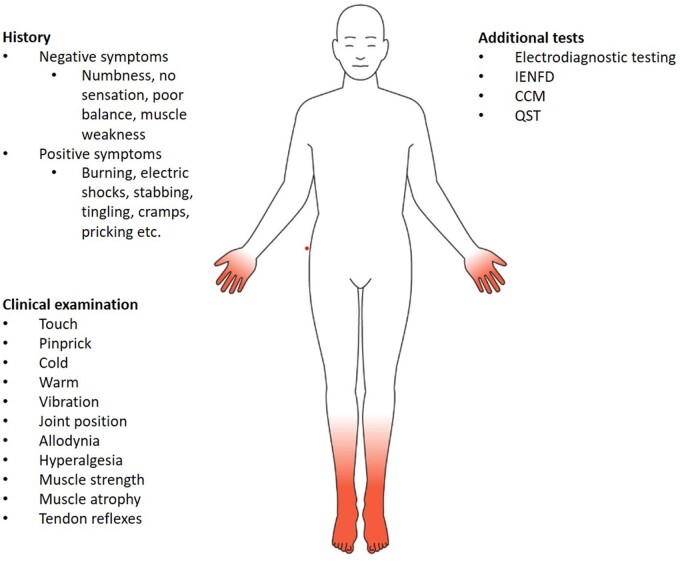
Peripheral neuropathy is one of the most common complications of both type 1 and type 2 diabetes. Up to half of patients with diabetes develop neuropathy during the course of their disease, which is accompanied by neuropathic pain in 30-40% of cases. Peripheral nerve injury in diabetes can manifest as progressive distal symmetric polyneuropathy, autonomic neuropathy, radiculo-plexopathies, and mononeuropathies. The most common diabetic neuropathy is distal symmetric polyneuropathy, which we will refer to as DN, with its characteristic glove and stocking like presentation of distal sensory or motor function loss. DN or its painful counterpart, painful DN, are associated with increased mortality and morbidity; thus, early recognition and preventive measures are essential. Nevertheless, it is not easy to diagnose DN or painful DN, particularly in patients with early and mild neuropathy, and there is currently no single established diagnostic gold standard. The most common diagnostic approach in research is a hierarchical system, which combines symptoms, signs, and a series of confirmatory tests. The general lack of long-term prospective studies has limited the evaluation of the sensitivity and specificity of new morphometric and neurophysiological techniques. Thus, the best paradigm for screening DN and painful DN both in research and in clinical practice remains uncertain. Herein, we review the diagnostic challenges from both clinical and research perspectives and their implications for managing patients with DN. There is no established DN treatment, apart from improved glycaemic control, which is more effective in type 1 than in type 2 diabetes, and only symptomatic management is available for painful DN. Currently, less than one-third of patients with painful DN derive sufficient pain relief with existing pharmacotherapies. A more precise and distinct sensory profile from patients with DN and painful DN may help identify responsive patients to one treatment versus another. Detailed sensory profiles will lead to tailored treatment for patient subgroups with painful DN by matching to novel or established DN pathomechanisms and also for improved clinical trials stratification. Large randomized clinical trials are needed to identify the interventions, i.e. pharmacological, physical, cognitive, educational, etc., which lead to the best therapeutic outcomes.
Keywords: diabetic neuropathy; diagnostic challenges; implication for management; painful diabetic neuropathy.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Baldereschi M, Inzitari M, Di Carlo A, Farchi G, Scafato E, Inzitari D.; ILSA Working Group. Epidemiology of distal symmetrical neuropathies in the Italian elderly. Neurology. 2007;68(18):1460–1467. - PubMed
-
- Hanewinckel R, Drenthen J, van Oijen M, Hofman A, van Doorn PA, Ikram MA.. Prevalence of polyneuropathy in the general middle-aged and elderly population. Neurology. 2016;87(18):1892–1898. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
