

Decompressive craniectomy combined with mild hypothermia in patients with large hemispheric infarction: a randomized controlled trial
- PMID: 33711963
- PMCID: PMC7953537
- DOI: 10.1186/s12883-021-02142-7
Decompressive craniectomy combined with mild hypothermia in patients with large hemispheric infarction: a randomized controlled trial
Abstract
Background: The effect of hypothermia on large hemispheric infarction (LHI) remains controversial. Our study aimed to explore the therapeutic outcomes of decompressive craniectomy (DC) combined with hypothermia on LHI.
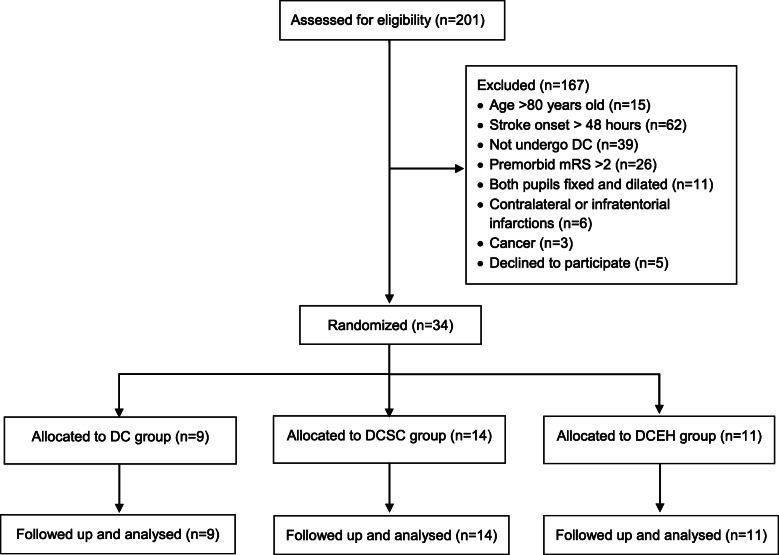
Methods: Patients were randomly divided into three groups: the DC group, the DC plus head surface cooling (DCSC) group and the DC plus endovascular hypothermia (DCEH) group. The DC group was maintained normothermia. The DCSC group received 24-h ice cap on the head for 7 days. While the DCEH group were given endovascular hypothermia (34 °C). Mortality and modified Rankin Scale (mRS) score at 6 months were evaluated.
Results: Thirty-four patients were included in the study. Mortality of the DC, DCSC and DCEH groups at discharge were 22.2% (2/9), 0% (0/14) and 9.1% (1/11), respectively. However, it increased to 44.4% (4/9), 21.4% (3/14) and 45.5% (5/11) at 6 months, respectively (p = 0.367). Pneumonia (8 cases) was the leading cause of death after discharge. Twelve cases (35.3%) achieved good neurological outcome (mRS 0-3) at 6 months. The proportions of good neurological outcome in the DC, DCSC and DCEH groups were 22.2% (2/9 cases), 42.9% (6/14 cases) and 36.4% (4/11), respectively. The DCSC group seemed to have higher proportion of good outcomes, but there was no significant difference between groups (p = 0.598). Among survivors, endovascular hypothermia had a higher proportion of good outcome (DC group, 2/5 cases, 40.0%; DCSC group, 6/11 cases, 54.5%; DCEH group, 4/6 cases, 66.7%; p = 0.696). The incidence of complications in the DCEH group was higher than those of the DC and DCSC groups (18.9%, 12.0%, and 12.1%, respectively; p = 0.025).
Conclusions: There is still no evidence to confirm that hypothermia further reduces long-term mortality and improves neurological outcomes in LHI patients with DC. However, there is a trend to benefit survivors from hypothermia. A local cooling method may be a better option for DC patients, which has little impact on systematic complications.
Trial registration: Decompressive Hemicraniectomy Combined Hypothermia in Malignant Middle Cerebral Artery Infarct, ChiCTR-TRC-12002698. Registered 11 Oct 2012- Retrospectively registered, URL: http://www.chictr.org.cn/showproj.aspx?proj=6854 .
Keywords: Decompressive craniectomy; Large hemispheric infarction; Neurological outcome; Randomized controlled trial; Target temperature management.
Conflict of interest statement
There is no conflict of interest to disclosure.
Figures

References
-
- Vahedi K, Vicaut E, Mateo J, Kurtz A, Orabi M, Guichard JP, et al. Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECIMAL trial) Stroke. 2007;38(9):2506–2517. doi: 10.1161/STROKEAHA.107.485235. - DOI - PubMed
-
- Hofmeijer J, Kappelle LJ, Algra A, Amelink GJ, van Gijn J, van der Worp HB, et al. Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy after middle cerebral artery infarction with life-threatening edema trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol. 2009;8(4):326–333. doi: 10.1016/S1474-4422(09)70047-X. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
