

Predictive value of C-reactive protein to albumin ratio as a biomarker for initial and repeated intravenous immunoglobulin resistance in a large cohort of Kawasaki disease patients: a prospective cohort study
- PMID: 33712036
- PMCID: PMC7953655
- DOI: 10.1186/s12969-021-00517-1
Predictive value of C-reactive protein to albumin ratio as a biomarker for initial and repeated intravenous immunoglobulin resistance in a large cohort of Kawasaki disease patients: a prospective cohort study
Abstract
Background: Intravenous immunoglobulin (IVIG) resistance prediction is one pivotal topic of interests in Kawasaki disease (KD). This study aimed to prospectively investigated the value of C-reactive protein-to-albumin (CAR) in predicting both initial and repeated IVIG resistance in patients with KD, and to test the hypothesis that CAR was more valuable or accurate than either C-reactive protein (CRP) or albumin (ALB) alone in IVIG resistance prediction.
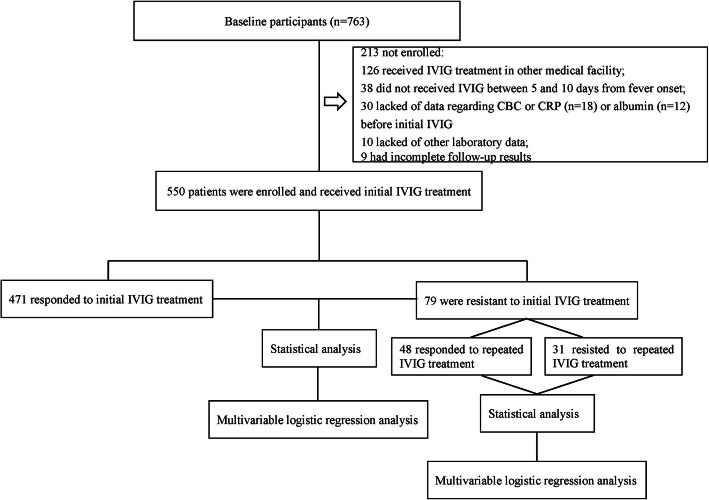
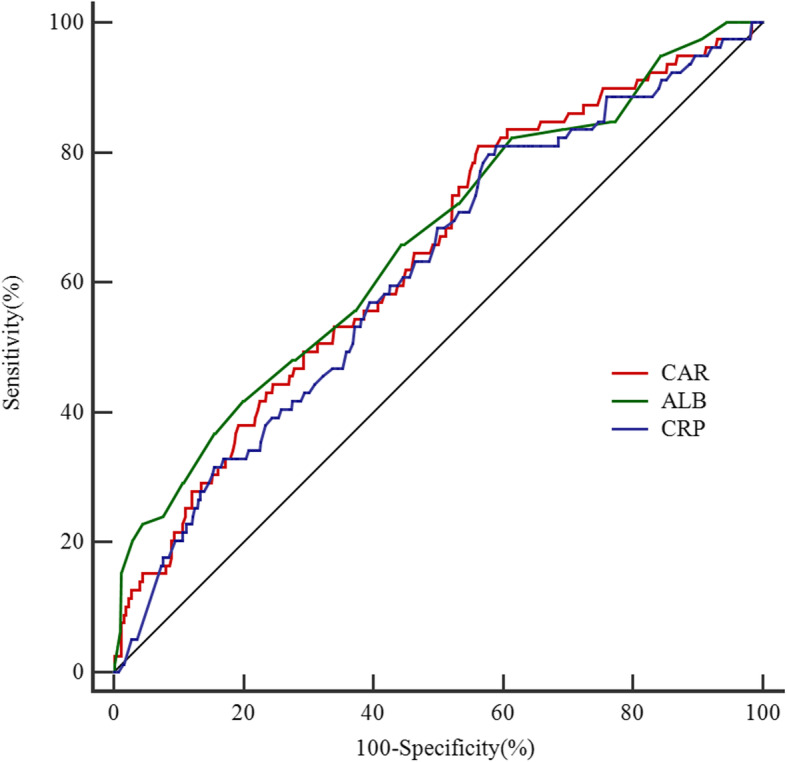
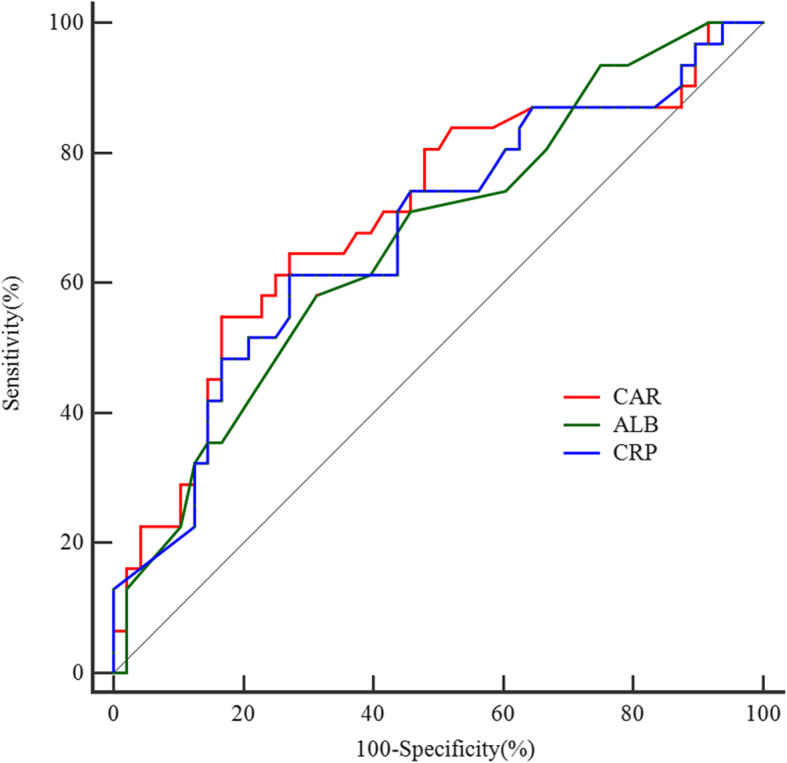
Method: A prospective cohort study involving 550 patients with KD was conducted. The clinical and laboratory data were compared between IVIG-response group and IVIG-resistance group. Multivariate logistic regression analysis was performed to identify the independent risk factors of initial/repeated IVIG resistance. Receiver operating characteristic (ROC) curves analysis was applied to assess the validity of CAR, CRP and ALB in predicting both initial and repeated IVIG resistance.
Results: CAR was significantly higher in IVIG non-responders and was identified as independent risk factor for both initial and repeated IVIG resistance in KD. The best cut-off value of CAR for initial and repeated IVIG resistance prediction was 2.07 and 3.34, with a corresponding sensitivity of 0.610 and 0.548, a specificity of 0.552 and 0.813, respectively. The value of CAR was not better than either CRP or ALB alone for both initial and repeated IVIG resistance prediction.
Conclusion: A higher CAR was an independent risk factor for both initial and repeated IVIG resistance. However, similar with that of CRP or ALB, the predictive value of CAR was not good enough for both initial and repeated IVIG resistance prediction in KD.
Keywords: C-reactive protein to albumin ratio; Intravenous immunoglobulin resistance; Kawasaki disease.
Conflict of interest statement
None of authors declared any conflict of interests.
Figures
Comment in
-
Letter to the editor regarding "Value of C-reactive protein/albumin ratio in predicting intravenous immunoglobulin-resistant Kawasaki disease - A data from multi-institutional study in China".Int Immunopharmacol. 2021 Jun;95:107631. doi: 10.1016/j.intimp.2021.107631. Epub 2021 Apr 23. Int Immunopharmacol. 2021. PMID: 33896753 No abstract available.
Similar articles
-
Predictive value of Albumin-Bilirubin grade for intravenous immunoglobulin resistance in a large cohort of patients with Kawasaki disease: a prospective study.Pediatr Rheumatol Online J. 2021 Sep 25;19(1):147. doi: 10.1186/s12969-021-00638-7. Pediatr Rheumatol Online J. 2021. PMID: 34563210 Free PMC article.
-
Predictive value of lymphocyte-to-C-reactive protein ratio for predicting initial and repeated intravenous immunoglobulin resistance in a large cohort of Kawasaki disease: a prospective cohort study.Eur J Pediatr. 2025 Jul 9;184(8):472. doi: 10.1007/s00431-025-06296-1. Eur J Pediatr. 2025. PMID: 40632184
-
Predictive value of serum procalcitonin for both initial and repeated immunoglobulin resistance in Kawasaki disease: a prospective cohort study.Pediatr Rheumatol Online J. 2019 Nov 27;17(1):78. doi: 10.1186/s12969-019-0379-5. Pediatr Rheumatol Online J. 2019. PMID: 31775782 Free PMC article.
-
Predictors of intravenous immunoglobulin-resistant Kawasaki disease in children: a meta-analysis of 4442 cases.Eur J Pediatr. 2018 Aug;177(8):1279-1292. doi: 10.1007/s00431-018-3182-2. Epub 2018 Jun 8. Eur J Pediatr. 2018. PMID: 29948255 Free PMC article. Review.
-
Nutrition-Associated Biomarkers in Predicting Intravenous Immunoglobulin Resistance and Coronary Artery Lesions in Kawasaki Disease: A Systematic Review and Meta-Analysis.Food Sci Nutr. 2024 Dec 15;13(1):e4647. doi: 10.1002/fsn3.4647. eCollection 2025 Jan. Food Sci Nutr. 2024. PMID: 39803242 Free PMC article. Review.
Cited by
-
Analysis and validation of clinical subgroups of Kawasaki disease in children in China: a retrospective study.BMJ Paediatr Open. 2024 Oct 15;8(1):e002650. doi: 10.1136/bmjpo-2024-002650. BMJ Paediatr Open. 2024. PMID: 39414342 Free PMC article.
-
A machine learning-based model to predict intravenous immunoglobulin resistance in Kawasaki disease.iScience. 2025 Feb 11;28(3):112004. doi: 10.1016/j.isci.2025.112004. eCollection 2025 Mar 21. iScience. 2025. PMID: 40109376 Free PMC article.
-
Prediction of coronary artery lesions based on C-reactive protein levels in children with Kawasaki Disease: a retrospective cohort study.J Pediatr (Rio J). 2023 Jul-Aug;99(4):406-412. doi: 10.1016/j.jped.2023.02.005. Epub 2023 Mar 25. J Pediatr (Rio J). 2023. PMID: 36977496 Free PMC article.
-
Value of blood inflammatory markers for predicting intravenous immunoglobulin resistance in Kawasaki disease: A systematic review and meta-analysis.Front Pediatr. 2022 Aug 23;10:969502. doi: 10.3389/fped.2022.969502. eCollection 2022. Front Pediatr. 2022. PMID: 36081627 Free PMC article.
-
Overexpressed Neuropilin-1 in Endothelial Cells Promotes Endothelial Permeability through Interaction with ANGPTL4 and VEGF in Kawasaki Disease.Mediators Inflamm. 2021 Aug 13;2021:9914071. doi: 10.1155/2021/9914071. eCollection 2021. Mediators Inflamm. 2021. PMID: 34434074 Free PMC article.
References
-
- Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the committee on Rheumatic fever, endocarditis, and Kawasaki disease, council on cardiovascular disease in the young, American Heart Association. Pediatrics. 2004;114(6):1708–33. - PubMed
-
- Durongpisitkul K, Gururaj VJ, Park JM, Martin CF. The prevention of coronary artery aneurysm in Kawasaki disease: a Meta-analysis on the efficacy of aspirin and immunoglobulin treatment. Pediatrics. 1995;96(6):1057–1061. - PubMed
-
- Uehara R, Belay ED, Maddox RA, Holman RC, Nakamura Y, Yashiro M, et al. Analysis of potential risk factors associated with nonresponse to initial intravenous immunoglobulin treatment among Kawasaki disease patients in Japan. Pediatr Infect Dis J. 2008;27(2):155–60. - PubMed
-
- Burns JC, Capparelli EV, Brown JA, Newburger JW, Glode MP, US/Canadian Kawasaki Syndrome Study Group. Intravenous gamma-globulin treatment and retreatment in Kawasaki disease. Pediatr Infect Dis J. 1998;17(12):1144–8. - PubMed
-
- Sundel RP, Beiser AS, Baker A, Burns JC, Newburger JW. Gamma globulin retreatment in Kawasaki disease. J Pediatr. 1993;123(4):657–9. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
