

Neurological symptoms in COVID-19: a cross-sectional monocentric study of hospitalized patients
- PMID: 33712089
- PMCID: PMC7953515
- DOI: 10.1186/s42466-021-00116-1
Neurological symptoms in COVID-19: a cross-sectional monocentric study of hospitalized patients
Abstract
Background: The SARS-Coronavirus-2 (SARS-CoV-2) invades the respiratory system, causing acute and sometimes severe pulmonary symptoms, but turned out to also act multisystematically with substantial impact on the brain. A growing number of studies suggests a diverse spectrum of neurological manifestations. To investigate the spectrum of symptoms, we here describe the neurological manifestations and complications of patients with proven SARS-CoV-2 infection who have been hospitalized at the RWTH University Hospital Aachen, Germany.
Methods: Between March and September 2020, we evaluated common symptoms, clinical characteristics, laboratory (including cerebrospinal fluid (CSF) analysis), radiological, and electroencephalography (EEG) data from 53 patients admitted with a positive SARS-CoV-2 polymerase chain reaction (PCR). We used the Montreal Cognitive Assessment Test (MoCA) to screen for cognitive impairment, when feasible. We compared critically ill and non-critically ill patients categorized according to the presence of Acute Respiratory Distress Syndrome (ARDS).
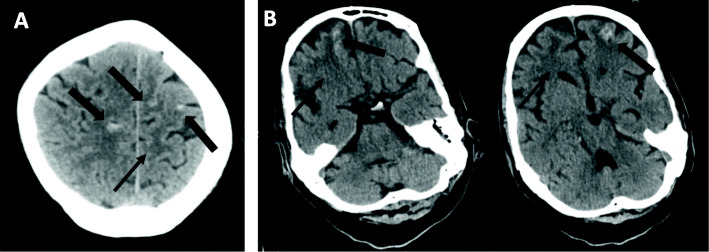
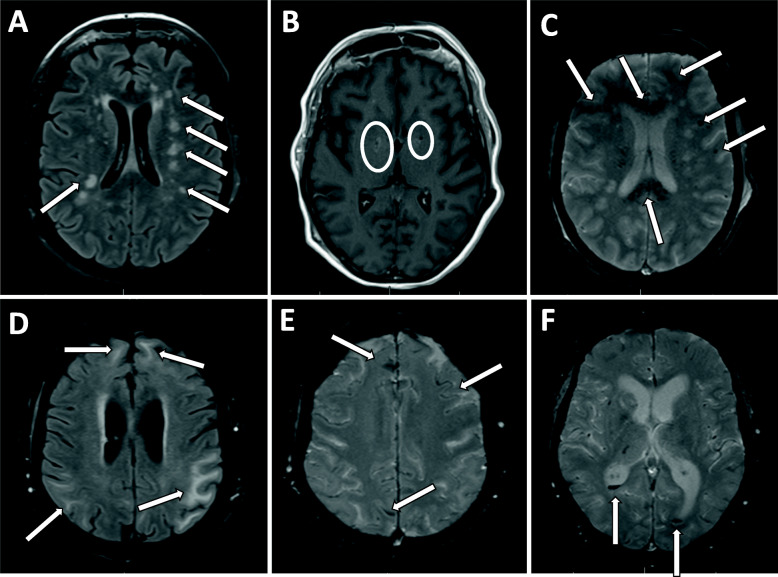
Results: Major clinical neurological features of hospitalized COVID-19 patients were coordination deficits (74%), cognitive impairment (61.5%), paresis (47%), abnormal reflex status (45%), sensory abnormalities (45%), general muscle weakness and pain (32%), hyposmia (26%), and headache (21%). Patients with ARDS were more severely affected than non-ADRS patients. 29.6% of patients with ARDS presented with subarachnoid bleedings, and 11.1% showed ischemic stroke associated with SARS-CoV-2 infection. Cognitive deficits mainly affected executive functions, attention, language, and delayed memory recall. We obtained cerebrospinal fluid (CSF) by lumbar puncture in nine of the 53 patients, none of which had a positive SARS-CoV-2 PCR.
Conclusions: In line with previous findings, our results provide evidence for a range of SARS-CoV-2-associated neurological manifestations. 26% of patients reported hyposmia, emphasizing the neuro-invasive potential of SARS-CoV-2, which can enter the olfactory bulb. It can therefore be speculated that neurological manifestations may be caused by direct invasion of the virus in the CNS; however, PCR did not reveal positive intrathecal SARS-CoV-2. Therefore, we hypothesize it is more likely that the para-infectious severe pro-inflammatory impact of COVID-19 is responsible for the neurological deficits including cognitive impairment. Future studies with comprehensive longitudinal assessment of neurological deficits are required to determine potential long-term complications of COVID-19.
Keywords: COVID-19; Cognitive impairment; Neuro-invasive potential; Neurological symptoms; SARS-CoV-2.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous