

Interhospital failure to rescue after coronary artery bypass grafting
- PMID: 33712236
- PMCID: PMC8679510
- DOI: 10.1016/j.jtcvs.2021.01.064
Interhospital failure to rescue after coronary artery bypass grafting
Abstract
Objective: We evaluated whether interhospital variation in mortality rates for coronary artery bypass grafting was driven by complications and failure to rescue.
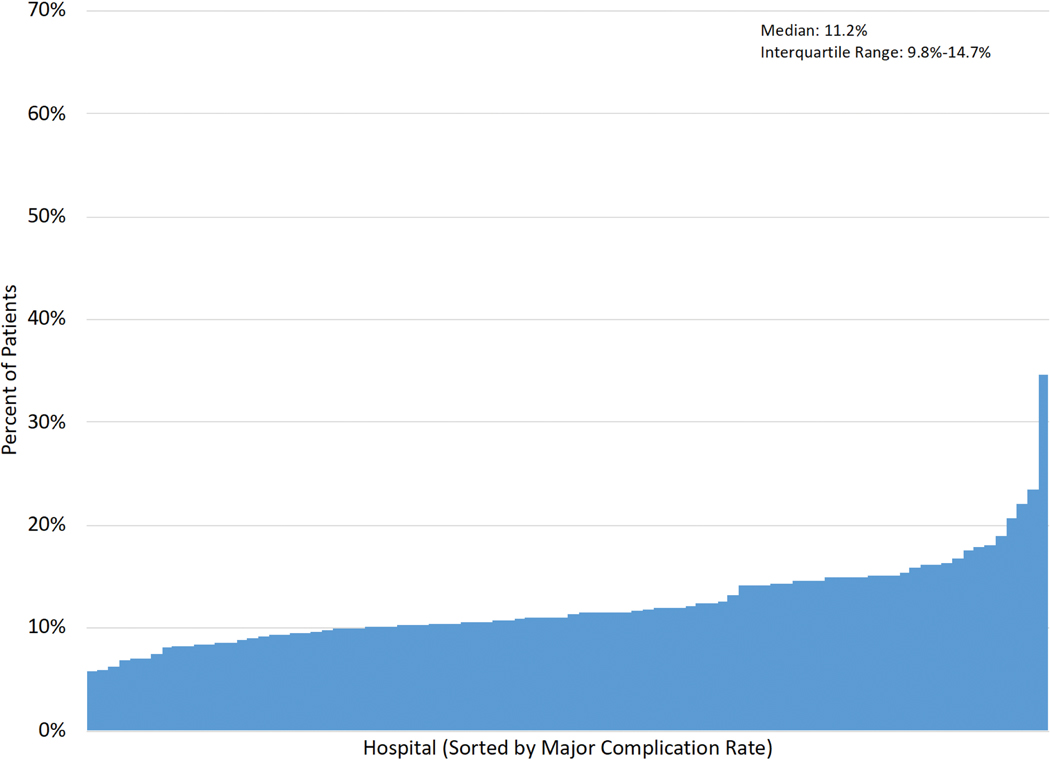
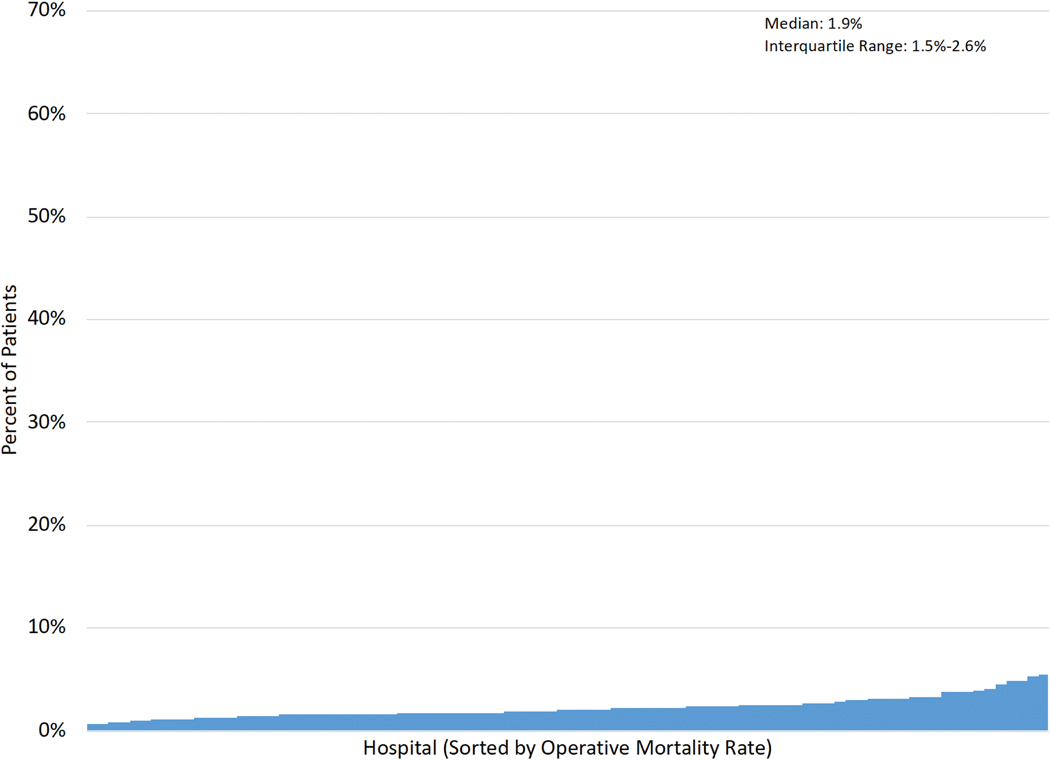
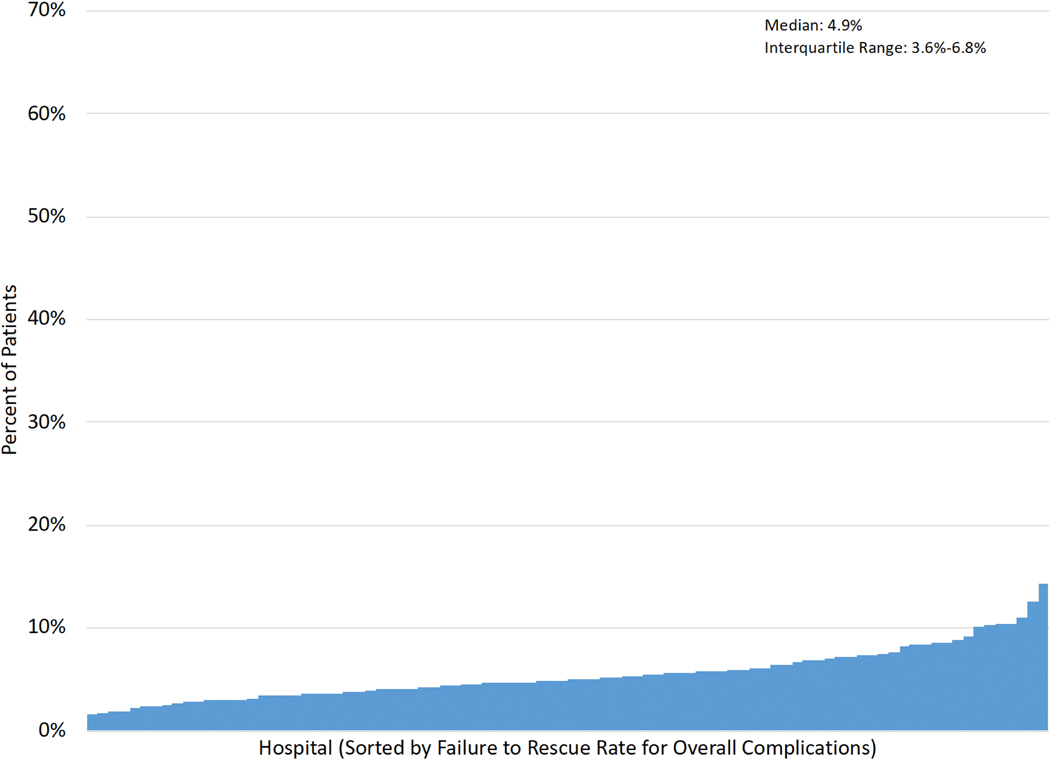
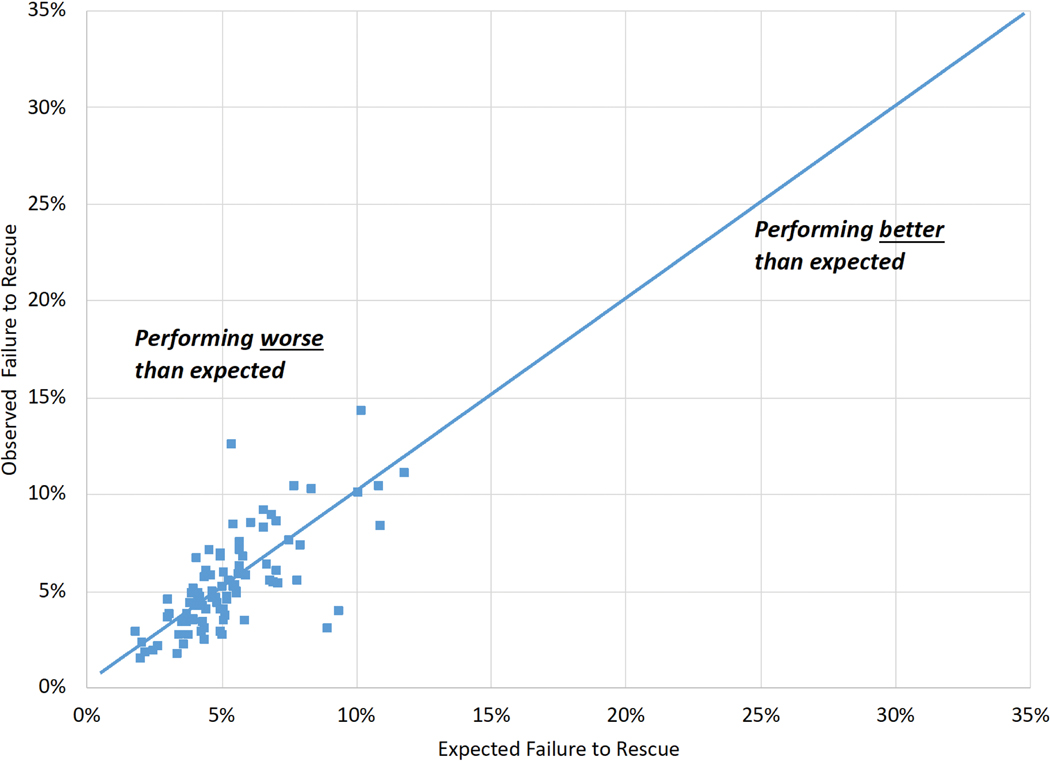
Methods: An observational study was conducted among 83,747 patients undergoing isolated coronary artery bypass grafting between July 2011 and June 2017 across 90 hospitals. Failure to rescue was defined as operative mortality among patients developing complications. Complications included the Society of Thoracic Surgeons 5 major complications (stroke, surgical reexploration, deep sternal wound infection, renal failure, prolonged intubation) and a broader set of 19 overall complications. After creating terciles of hospital performance (based on observed:expected mortality), each tercile was compared on the basis of crude rates of (1) major and overall complications, (2) operative mortality, and (3) failure to rescue (among major and overall complications). The correlation between hospital observed and expected (to address confounding) failure to rescue rates was assessed.
Results: Median Society of Thoracic Surgeons predicted mortality risk was similar across hospital observed:expected mortality terciles (P = .831). Mortality rates significantly increased across terciles (low tercile: 1.4%, high tercile: 2.8%). Although small in magnitude, rates of major (low tercile: 11.1%, high tercile: 12.2%) and overall (low tercile: 36.6%, high tercile: 35.3%) complications significantly differed across terciles. Nonetheless, failure to rescue rates increased substantially across terciles among patients with major (low tercile: 9.1%, high tercile: 14.3%) and overall (low tercile: 3.3%, high tercile: 6.8%) complications. Hospital observed and expected failure to rescue rates were positively correlated among patients with major (R2 = 0.14) and overall (R2 = 0.51) complications.
Conclusions: The reported interhospital variability in successful rescue after coronary artery bypass grafting supports the importance of identifying best practices at high-performing hospitals, including early recognition and management of complications.
Keywords: complications; coronary artery bypass grafting; mortality.
Copyright © 2021 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest: None
Figures






Comment in
-
Commentary: Failure to rescue: "The medium is the message".J Thorac Cardiovasc Surg. 2023 Jan;165(1):144-145. doi: 10.1016/j.jtcvs.2021.01.107. Epub 2021 Feb 3. J Thorac Cardiovasc Surg. 2023. PMID: 33653605 No abstract available.
-
Commentary: It takes a village: The next frontier in quality improvement.J Thorac Cardiovasc Surg. 2023 Jan;165(1):145-146. doi: 10.1016/j.jtcvs.2021.01.131. Epub 2021 Feb 5. J Thorac Cardiovasc Surg. 2023. PMID: 33685732 No abstract available.
-
Commentary: Failure to rescue: What does it really measure?J Thorac Cardiovasc Surg. 2023 Jan;165(1):146-148. doi: 10.1016/j.jtcvs.2021.01.129. Epub 2021 Feb 5. J Thorac Cardiovasc Surg. 2023. PMID: 33812683 No abstract available.
References
-
- Hospital Compare. Medicare.gov | Hospital Compare. Accessed October 16, 2020. https://www.medicare.gov/hospitalcompare/search.html?
-
- Homepage | STS. Accessed March 30, 2020. http://www.sts.org
-
- Edwards FH, Ferraris VA, Kurlansky PA, Lobbdell KW, He X, O’Brien SM, et al. Failure to Rescue Rates After Coronary Artery Bypass Grafting: An Analysis From The Society of Thoracic Surgeons Adult Cardiac Surgery Database. Ann Thorac Surg. 2016;102(2):458–464. - PubMed
-
- Shahian DM, O’Brien SM, Filardo G, Ferraris VA, Haan CK, Rich JB, et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 1--coronary artery bypass grafting surgery. Ann Thorac Surg. 2009;88(1 Suppl):S2–S22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
