

STAG2 as a prognostic biomarker in low-grade non-muscle invasive bladder cancer
- PMID: 33712344
- PMCID: PMC8286298
- DOI: 10.1016/j.urolonc.2021.02.007
STAG2 as a prognostic biomarker in low-grade non-muscle invasive bladder cancer
Abstract
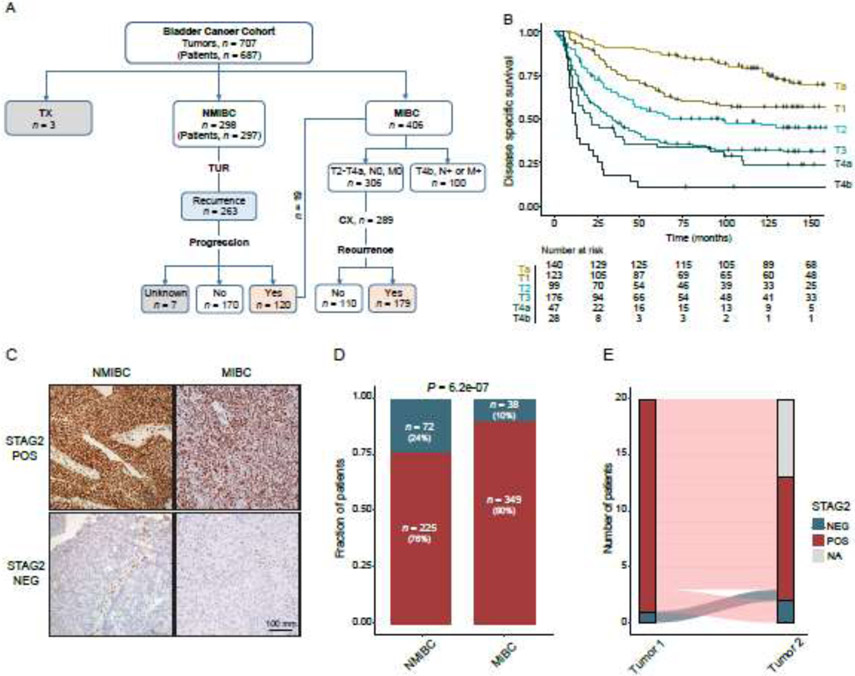
Objective: Improvements to bladder cancer risk stratification guidelines are needed to better tailor post-operative surveillance and adjuvant therapy to individual patients. We previously identified STAG2 as a commonly mutated tumor suppressor gene in bladder cancer and an independent predictor of progression in NMIBC. Here we test the value of combining STAG2 immunostaining with other risk stratification biomarkers in NMIBC, and as an individual biomarker in MIBC.
Materials and methods: STAG2 immunohistochemistry was performed on a progressor-enriched cohort of tumors from 297 patients with NMIBC, and on tumors from 406 patients with MIBC from Aarhus University Hospital in Denmark. Survival analysis was performed using Kaplan-Meier survival analysis, the log rank test, and Cox proportional hazards models.
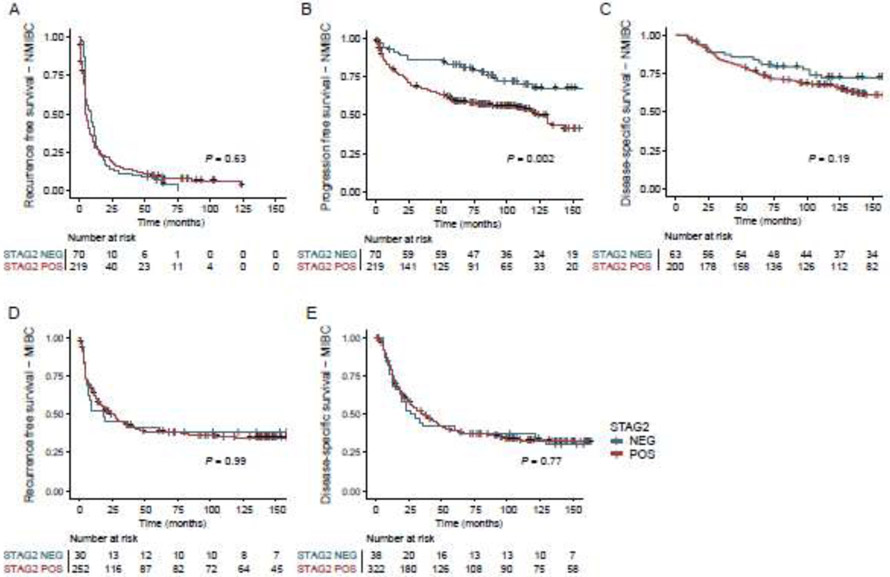
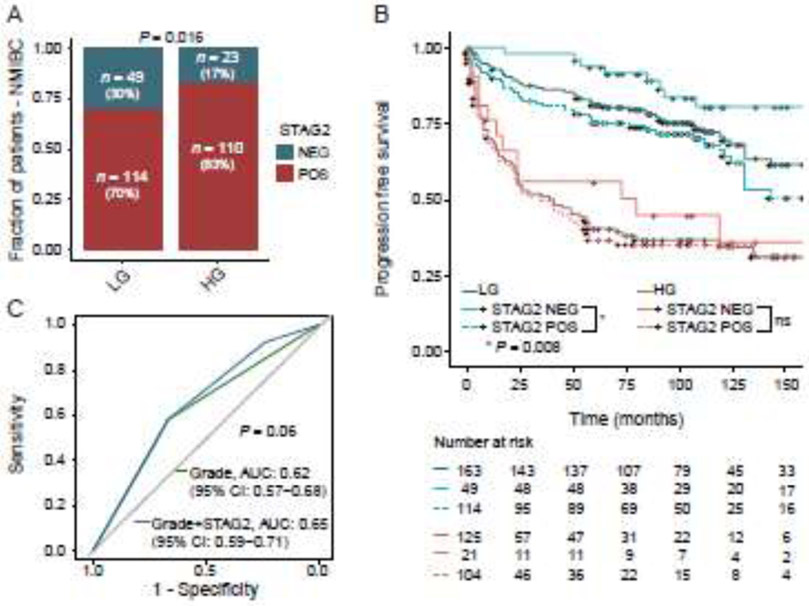
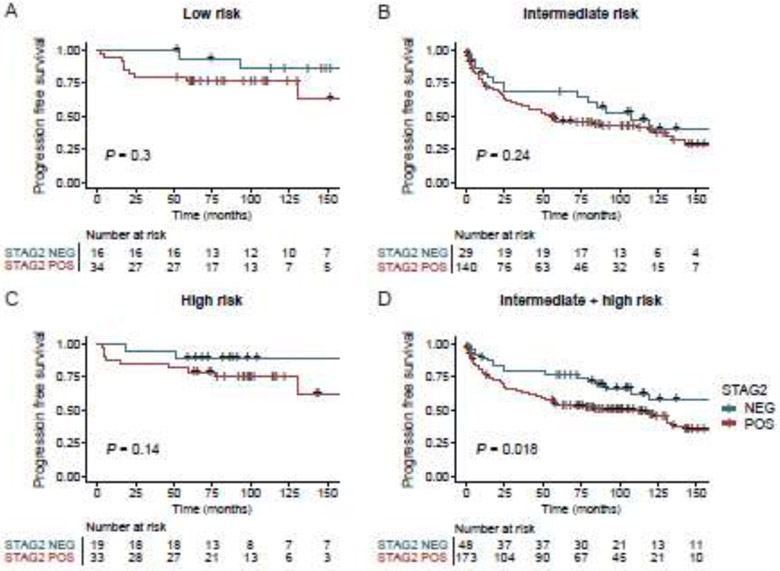
Results: STAG2-negative low-grade NMIBC tumors were 2.5 times less likely to progress to muscle invasion than STAG2-positive low-grade NMIBC tumors (Log-rank test, P = 0.008). In a composite group of patients with AUA intermediate and high-risk NMIBC tumors, STAG2-negative tumors were less likely to progress (Log-rank test, P = 0.02). In contrast to NMIBC, we show that STAG2 is not useful as a prognostic biomarker in MIBC.
Conclusions: STAG2 immunostaining can be used to subdivide low-grade NMIBC tumors into two groups with substantially different risks of disease progression. Furthermore, STAG2 immunostaining may be useful to enhance NMIBC risk stratification guidelines, though larger cohorts are needed to solidify this conclusion in individual risk groups. STAG2 is not useful as a biomarker in MIBC. Further study of the use of STAG2 immunostaining as a biomarker for predicting the clinical behavior in NMIBC is warranted.
Keywords: Bladder cancer; Bladder cancer recurrence and progression; Risk stratification guidelines; STAG2.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
References
-
- National Cancer Institute, National Institutes of Health. Cancer Stat Facts: Bladder Cancer https://seer.cancer.gov/statfacts/html/urinb.html; [accessed 19 January 2021].
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
