

Treatment approach and survival from glioblastoma: results from a population-based retrospective cohort study from Western Norway
- PMID: 33712524
- PMCID: PMC7959220
- DOI: 10.1136/bmjopen-2020-043208
Treatment approach and survival from glioblastoma: results from a population-based retrospective cohort study from Western Norway
Abstract
Objectives: To evaluate treatment and survival from glioblastoma in a real-world setting.
Design and settings: A population-based retrospective cohort study from Western Norway.
Participants: 363 patients aged 18 years or older diagnosed with glioblastoma between 1 January 2007 and 31 December 2014.
Primary and secondary outcome measures: Overall survival and survival rates determined by Kaplan-Meier method, groups compared by log-rank test. Associations between clinical characteristics and treatment approach assessed by logistic regression. Associations between treatment approach and outcome analysed by Cox regression.
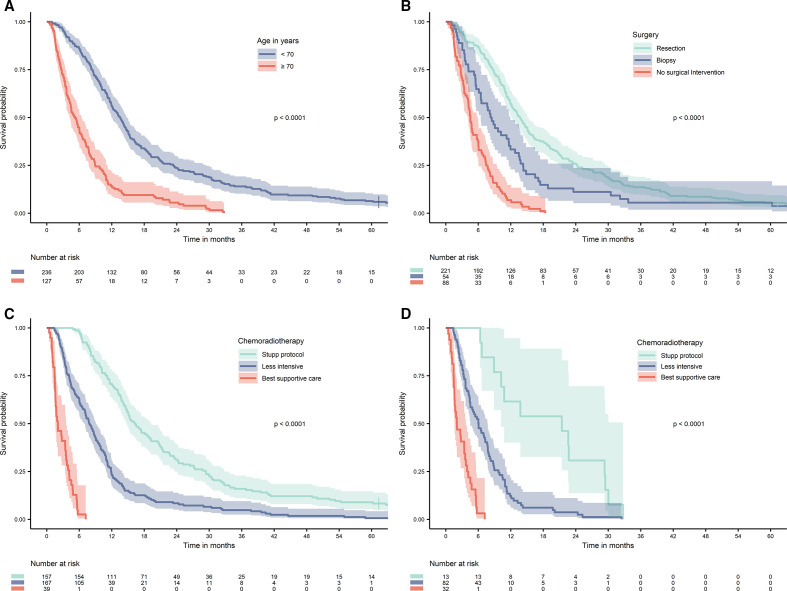
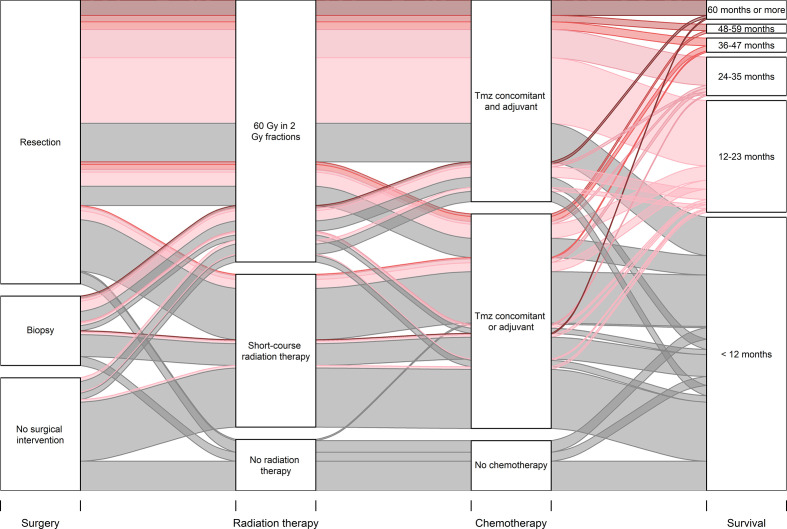
Results: Median overall survival was 10.2 months (95% CI 9.1 to 11.3). Resection was performed in 221 patients (60.9%), and was inversely associated with age over 70 years, higher comorbidity burden, deep-seated tumour localisation and multifocality. Median survival was 13.7 months (95% CI 12.1 to 15.4) in patients undergoing tumour resection, 8.3 months (95% CI 6.6 to 9.9) in patients undergoing biopsy and 4.5 months (95% CI 4.0 to 5.1) in patients where no surgical intervention was performed. Chemoradiotherapy according to the Stupp protocol was given to 157 patients (43%). Age over 70 years, higher comorbidity burden and cognitive impairment were associated with less intensive chemoradiotherapy. Median survival was 16.3 months (95% CI 14.1 to 18.5), 7.9 months (95% CI 6.7 to 9.0) and 2.0 months (95% CI 0.9 to 3.2) in patients treated according to the Stupp protocol, with less intensive chemoradiotherapy and with best supportive care, respectively. Surgical resection (HR 0.61 (95% CI 0.47 to 0.79)) and chemoradiotherapy according to the Stupp protocol (HR 0.09 (95% CI 0.06 to 0.15)) were strongly associated with favourable overall survival, when adjusted for clinical variables.
Conclusions: In a real-world setting, less than half of the patients received full-course chemoradiotherapy, with a median survival comparable to results from clinical trials. Survival was considerably worse in patients receiving less intensive treatment. Our results point out a substantial risk of undertreating glioblastoma, especially in elderly patients.
Keywords: adult oncology; chemotherapy; neurological oncology; radiation oncology.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical