

Point-of-care SARS-CoV-2 serological assays for enhanced case finding in a UK inpatient population
- PMID: 33712679
- PMCID: PMC7955061
- DOI: 10.1038/s41598-021-85247-w
Point-of-care SARS-CoV-2 serological assays for enhanced case finding in a UK inpatient population
Abstract
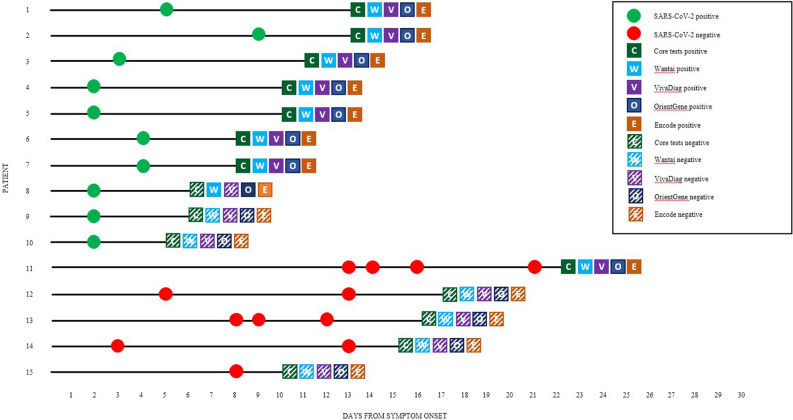
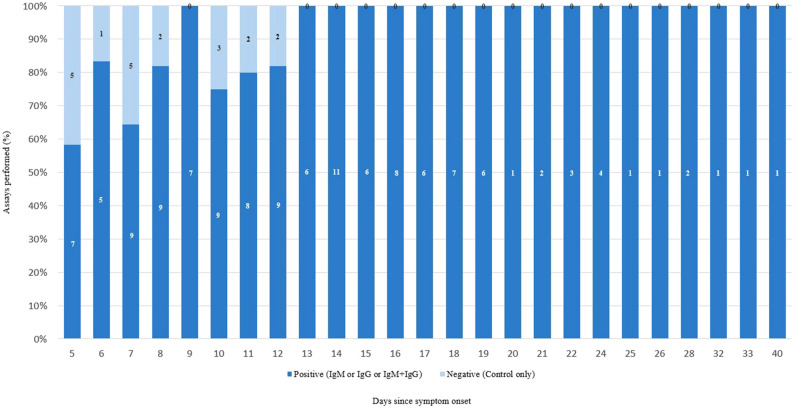
Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2) has become a global pandemic. Case identification is currently made by real-time polymerase chain reaction (PCR) during the acute phase and largely restricted to healthcare laboratories. Serological assays are emerging but independent validation is urgently required to assess their utility. We evaluated five different point-of-care (POC) SARS-CoV-2 antibody test kits against PCR, finding concordance across the assays (n = 15). We subsequently tested 200 patients using the OrientGene COVID-19 IgG/IgM Rapid Test Cassette and find a sensitivity of 74% in the early infection period (day 5-9 post symptom onset), with 100% sensitivity not seen until day 13, demonstrating inferiority to PCR testing in the infectious period. Negative rate was 96%, but in validating the serological tests uncovered potential false-negatives from PCR testing late-presenting cases. A positive predictive value (PPV) of 37% in the general population precludes any use for general screening. Where a case definition is applied however, the PPV is substantially improved (95.4%), supporting use of serology testing in carefully targeted, high-risk populations. Larger studies in specific patient cohorts, including those with mild infection are urgently required to inform on the applicability of POC serological assays to help control the spread of SARS-CoV-2 and improve case finding of patients that may experience late complications.
Conflict of interest statement
LSPM has consulted and/or received speaker fees from bioMerieux (2013–2020), Pfizer (2018–2020), Eumedica (2016–2020), Umovis Lab (2020), DNAelectronics (2015–18), and Dairy Crest (2017–2018), received research grants from the National Institute for Health Research (2013–2019), and CW + Charity (2018–2020). NM has received speaker fees from Beyer (2016) and Pfizer (2019–2020) and received educational support from Eumedica (2016) and Baxter (2017). JS, the Editor-in-Chief of Oncogene has sat on Scientific Advisory Boards for Celltrion, Singapore Biotech, Vor Biopharma, Vaccitech, Heat Biologics, Lilly, Greenmantle and Benevolent AI, has consulted with Lansdowne partners and Vitruvian. He sits on the Board of Directors for BB Biotech Healthcare Trust. SJCP has received a research grant from the Scientific Exploration Society. EC has received speaker fees from bioMerieux (2019). The other authors declare no competing interests.
Figures

References
-
- Zhang, Y.-Z. Novel 2019 coronavirus genome. In Virological (accessed 28 March 2020); http://virological.org/t/novel-2019-coronavirus-genome/319.
-
- Luan RS, Wang X, Sun X, et al. Epidemiology, treatment, and epidemic prevention and control of the coronavirus disease 2019: A review. Sichaun Da Xue Xue Bao Yi Yue Ban. 2020;51(2):131–138. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
