

Maximum vasoactive-inotropic score and mortality in extremely premature, extremely low birth weight infants
- PMID: 33712712
- PMCID: PMC8435049
- DOI: 10.1038/s41372-021-01030-9
Maximum vasoactive-inotropic score and mortality in extremely premature, extremely low birth weight infants
Abstract
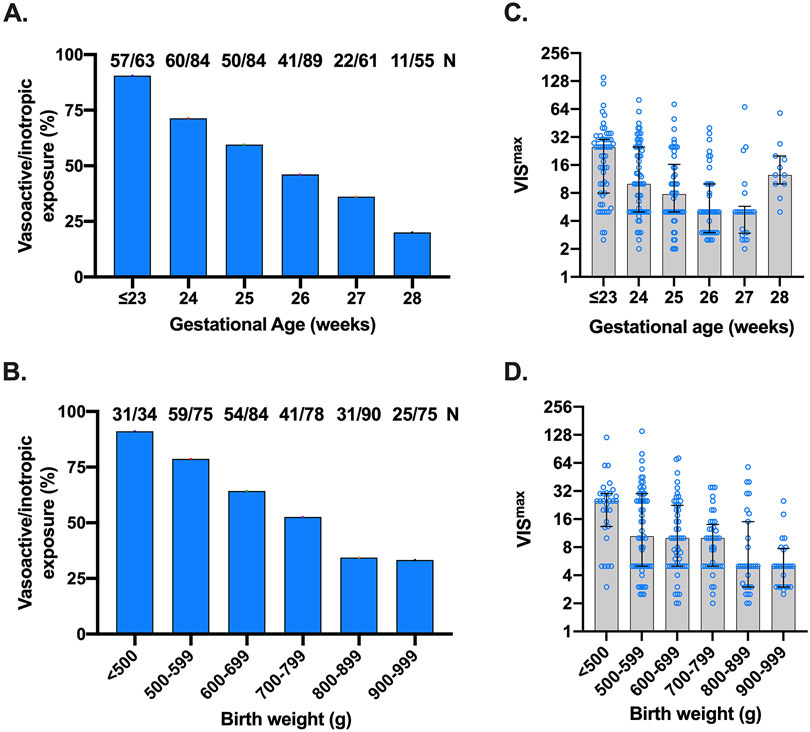
Objective: To determine the relationship between maximum vasoactive-inotropic (VISmax) and mortality in extremely premature (<29 weeks completed gestation), extremely low birth weight (ELBW, <1000 g) infants.
Study design: Single center, retrospective, and observational cohort study.
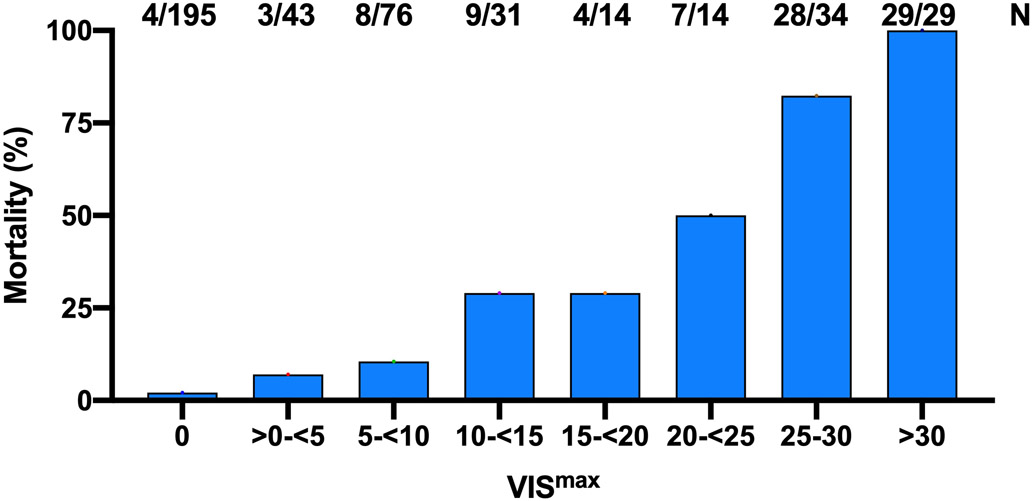
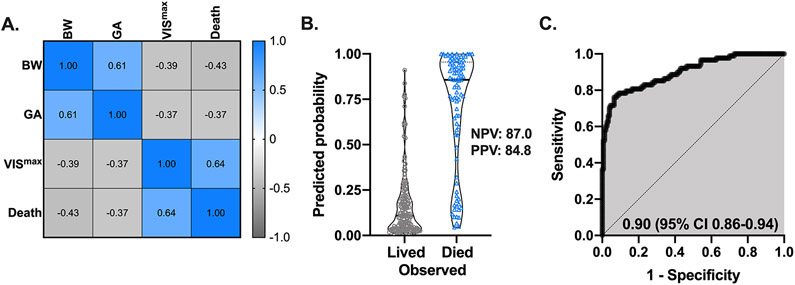
Results: We identified 436 ELBW, <29 week, inborn infants cared for during the study period. Compared to infants with VISmax of 0, the frequency of mortality based on VISmax ranged from 3.3-fold to 46.1-fold. VISmax > 30 was associated with universal mortality. Multivariable modeling that included gestational age, birth weight, and VISmax revealed significant utility to predict mortality with negative predictive value of 87.0% and positive predictive value of 84.8% [adjusted AUROC: 0.90, (0.86-0.94)] among patients that received vasoactive-inotropic treatment.
Conclusion: VISmax is an objective measure of hemodynamic/cardiovascular support that was directly associated with mortality in extremely premature ELBW infants. The VISmax represents an important step towards neonatal precision medicine and risk stratification of extremely premature ELBW infants.
© 2021. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Figures
Similar articles
-
A new mortality score in preterm infants: the vasoactive inotropic score.BMC Pediatr. 2025 Apr 23;25(1):317. doi: 10.1186/s12887-025-05638-0. BMC Pediatr. 2025. PMID: 40264079 Free PMC article.
-
Validity of the vasoactive-inotropic score in preterm neonates receiving cardioactive therapies.Early Hum Dev. 2022 Oct;173:105657. doi: 10.1016/j.earlhumdev.2022.105657. Epub 2022 Aug 20. Early Hum Dev. 2022. PMID: 36087459
-
Obstetrical factors for death and brain injury among extremely-low-birth-weight infants.J Perinat Med. 2007;35(6):543-9. doi: 10.1515/JPM.2007.111. J Perinat Med. 2007. PMID: 18052840
-
Outcome of infants born preterm, with special emphasis on extremely low birthweight infants.Baillieres Clin Obstet Gynaecol. 1993 Sep;7(3):611-31. doi: 10.1016/s0950-3552(05)80451-1. Baillieres Clin Obstet Gynaecol. 1993. PMID: 7504603 Review.
-
Skin Care for the Extremely Low-Birthweight Infant.Neoreviews. 2023 Apr 1;24(4):e229-e242. doi: 10.1542/neo.24-4-e229. Neoreviews. 2023. PMID: 37002398 Review.
Cited by
-
Markers of platelet activation foR identification of late onset sEpsis in infaNTs: PARENT study protocol.Pediatr Res. 2024 Feb;95(3):852-856. doi: 10.1038/s41390-023-02812-x. Epub 2023 Sep 27. Pediatr Res. 2024. PMID: 37758864
-
Interaction of hydrocortisone and illness severity on head growth in cohort of ELBW infants.Pediatr Res. 2023 Dec;94(6):1958-1965. doi: 10.1038/s41390-023-02689-w. Epub 2023 Jun 20. Pediatr Res. 2023. PMID: 37340101 Free PMC article.
-
Perioperative hemodynamic parameters monitored by three noninvasive technologies in children with congenital heart disease: A prospective study.Pediatr Discov. 2024 Sep 12;3(2):e2505. doi: 10.1002/pdi3.2505. eCollection 2025 Jun. Pediatr Discov. 2024. PMID: 40666236 Free PMC article.
-
Echocardiography performed by the neonatologist: the impact on the clinical management.Pediatr Res. 2023 Aug;94(2):724-729. doi: 10.1038/s41390-023-02526-0. Epub 2023 Feb 18. Pediatr Res. 2023. PMID: 36807613
-
The association of vasoactive-inotropic score and surgical patients' outcomes: a systematic review and meta-analysis.Syst Rev. 2024 Jan 6;13(1):20. doi: 10.1186/s13643-023-02403-1. Syst Rev. 2024. PMID: 38184601 Free PMC article.
References
-
- Watkins PL, Dagle JM, Bell EF, Colaizy TT. Outcomes at 18 to 22 Months of Corrected Age for Infants Born at 22 to 25 Weeks of Gestation in a Center Practicing Active Management. J Pediatr 2020, 217: 52–58 e51. - PubMed
-
- Wernovsky G, Wypij D, Jonas RA, Mayer JE Jr., Hanley FL, Hickey PR, et al.Postoperative course and hemodynamic profile after the arterial switch operation in neonates and infants. A comparison of low-flow cardiopulmonary bypass and circulatory arrest. Circulation 1995, 92(8): 2226–2235. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
